Propensity Scores
A question that may arise from investigators who have not used propensity scores before is: Why must we estimate the probability that a subject receives a certain treatment since we know for certain which treatment was given?Õ An answer to this question is that if we use the probability that a subject would have been treated (that is, the propensity score) to adjust our estimate of the treatment e¤ect, we can create a Ôquasi-randomizedÕ experiment. That is, if we Þnd two subjects, one in the treated group and one in the control, with the same propensity score, then we could imagine that these two subjects were ÔrandomlyÕ assigned to each group in the sense of being equally likely to be treated or control. In a controlled experiment, the randomization, which assigns pairs of individuals to the treated and control groups, is better than this because it does not depend on the investigator conditioning on a particular set of covariates; rather it applies to any set of observed or unobserved covariates. Although the results of using the propensity scores are conditional only on the observed covariates, if one has the ability to measure many of the covariates that are believed to be related to the treatment assignment, then one can be fairly conÞdent that approximately unbiased estimates for the treatment e¤ect can be obtained.
Sir Austin Bradford Hill’s famous criteria for causality (for example, coherence, specificity, and a doseresponserelationship),
Braitman LE, Rosenbaum PR: Rare outcomes, common treatments: analytic strategies using propensity scores. Ann Intern Med 2002, 137:693-695. [PubMed Abstract] [Publisher Full Text] Localio AR, Berlin JA, Ten Have TR, Kimmel SE: Adjustments for center in multicenter studies: an overview. Ann Intern Med 2001, 135:112-123. [PubMed Abstract] [Publisher Full Text] Panageas KS, Schrag D, Riedel E, Bach PB, Begg CB: The effect of clustering of outcomes on the association of procedure volume and surgical outcomes. Ann Intern Med 2003, 139:658-665. [PubMed Abstract] [Publisher Full Text]
Methods
Gilbert and Lowenstein (Ann Emerg Med Volume 27, Issue 3, Pages 305-308 (March 1996))
{kind=link}
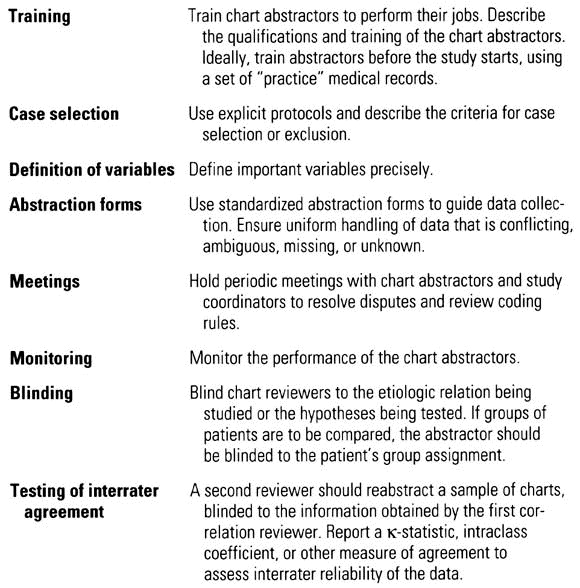
Worster A, Bledsoe RD, Cleve P, Fernandes CM, Upadhye S, Eva K. Reassessing the methods of medical record review studies in emergency medicine research. Ann Emerg Med. 2005;45:448451.
Worster A, Haines T. Advanced statistics: understanding medical record review (MRR) studies. Acad Emerg Med. 2004;11:187192.
From SGEM:
|
Method Criterion |
Answer |
|
|
1 |
Abstractors Training | Three abstractor were trained on 50 charts |
|
2 |
Case Selection Criteria | “Allergic Reaction” was the sole code available to physicians in their EMR |
|
3 |
Variable Definition | Very clear definitions were used |
|
4 |
Abstraction Forms | Standardized MS-Excel spread sheet |
|
5 |
Performance Monitoring | Weekly meetings |
|
6 |
Blind to Hypothesis | No, but all variables were entered before evaluation of the outcomes. |
|
7 |
IRR Mentioned | Yes |
|
8 |
IRR Tested | Yes, 5% of the cases were randomly selected and reviewed by second individual blinded to patient outcomes |
|
9 |
Medical Record Identified | Yes, EMR |
|
10 |
Sampling Method | Yes |
|
11 |
Missing Data | They describe how they dealt with missing data |
|
12 |
Ethics | Yes |