Musculoskeletal and Skin
Need an acoustic step-off. Make by using 10x strength jello.
abscess or cellulitis (or vascular aneurysm)
cellulitis looks like cobblestones, muscle with slight fluid
Epidermis/dermis®hypodermis®subcutaneous fascia®muscle®bone(shadows)
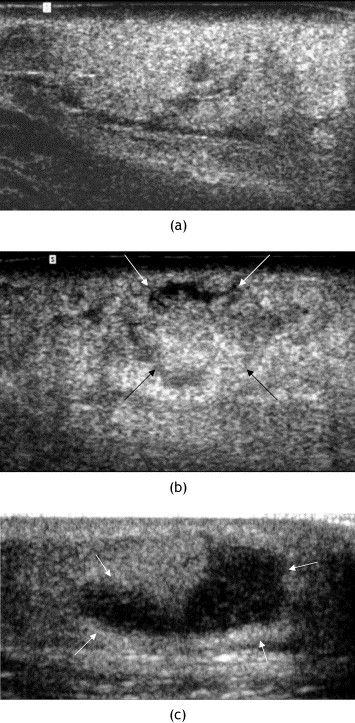
Abscess
Hypoechoic to anechoic, compressible, posteriro enhancement, no doppler flow
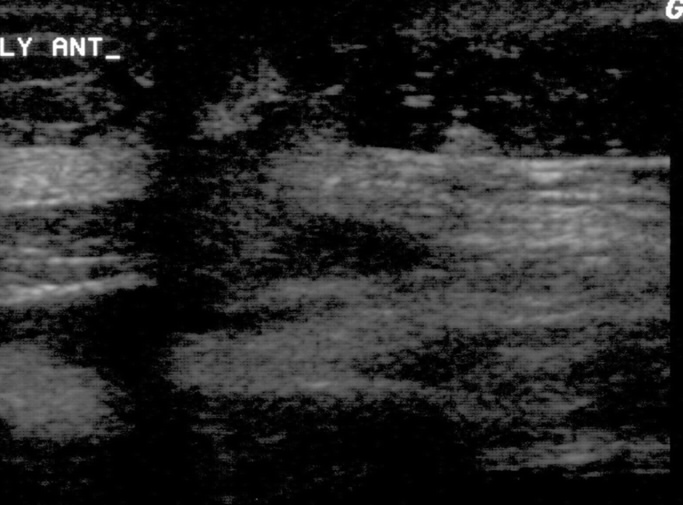
Cellulitis
looks just like other side but with more swelling
you will see cobblestoning
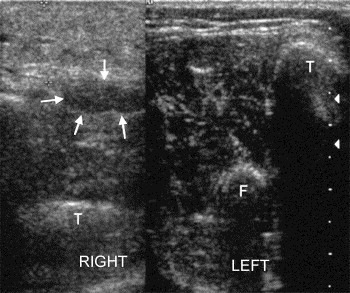
Necrotizing Fasciitis
abnormal thickening of fascia
irregularity
abnormal fluid collection along fascial plane (>4mm)
Joint Effusions
Look for the V which is where bone meets bone
Shoulder
go anterior
probe indicator horizontal
should see the biceps tendon in the bicipital groove
If there is fluid surrounding the tendon, then there is fluid in the joint
Knee
Go suprapatellar in longitudinal
will see the bursa which commicates with joint space, if more than a thin line then effusion
Hip
anterior oblique longitudinal on internally rotated leg
effusion if >5mm
Ankle
anterior tibiotalar recess
if capsule is displaced >3mm=effusion
Foreign Bodies
need stepoff pad
put dots on either side of the probe, can do it in 4 spots
Or put in transverse, use isosceles triangle rule. Measure distance down then go that far back and insert to 45 angle on either side of the probe while watching in real time. Then incise between the two needles.
Peritonsillar Abscess
use vaginal probe to get depth
then cut the needle cap to that length
Sinusitis
On maxillary sinus if you can see the apex of the sinus then there is sinusitis
Can also use waterbath to image extremities (The American Journal of Emergency Medicine Volume 22, Issue 7 , November 2004, Pages 589-593)
Standoffs:
Just heat some water and make a 10% solution of gelatin. You dont want to heat the water too much or you will burn the gelatin when you add it. Regular gelatin you make at home is less than 1% gelatin, you just need to concentrate it more. 10% means 100 mg per cc of liquid. For example, if you boil 1 liter of water, you need 100 gm of gelatin. Just do the math for whatever amount you need. You will need an electric mixer because this stuff is hard to dissolve, remember you are making a super-saturated solution (I bet you havent heard that word since the biochemistry days). Dont freeze it after you are done or it will crack, just put it in the refrigerator. It will last forever in the fridge, unless it contaminates. Just make sure the container is airtight so no evaporation occurs. Ive left the gelatin blocks out of the fridge (I actually put them in the closet), for about 5 days and they didnt melt and nothing grew on them. Gelatin is also used to make glue, so whatever container you use, make sure you clean it off right away or you will be scrubbing for a long time. The good news is that once you make the gelatin blocks, if they break you can just re-melt them and use them again, no need to mix or anything.
Musculoskeletal Infections
(Clin Rad 2005;60:149)
Can use it for anterior stab wounds as well

 Abscess
Abscess
 tensosynovitis
tensosynovitis
 nec fasc
nec fasc
 thrombosed vessel
thrombosed vessel
Ultrasound-guided hip arthrocentesis in the ED (The American Journal of Emergency Medicine Volume 25, Issue 1 , January 2007, Pages 80-86)
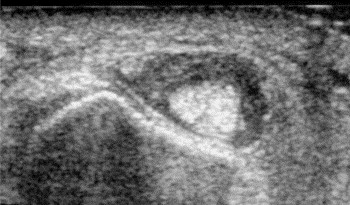
Tendon
Creating your own acoustic window enhanced your visualization of the superficial tendons and enabled you to see that your patient had sustained a large flexor tendon laceration. There is hypoechoic edema noted around the tendon in the sagittal plane, and you see a dark hypoechoic laceration traversing the fibrillar tendons on a longitudinal view (top). You scan through each tendon in both the axial and sagittal plane to ensure that the hypoechoic areas noted are not secondary to anisotropy (see Tips & Tricks below).Before you can finish saving the last image onto the machine for Q&A, your resident has already called back the hand surgeon to inform him that he hasn’t gotten off the hook quite so easily this time. As you wheel your handy ultrasound machine out of room 10, you can’t help but marvel at how “quick and minor” most problems can become with the help of bedside ultrasonography.Tips and Tricks | Evaluating Tendons Using Water Immersion 1. A careful history and physical exam will usually reveal whether tendon injury or disruption has occurred. Remember that normal motion can be seen on physical exam even with a 90% tendon disruption. Testing strength against resistance may help pick up a partial tendon injury that would be missed by range or motion assessment alone 2. Ultrasound can be used to augment clinical findings and help expedite the diagnosis, especially when the physical exam may be limited secondary to pain, swelling, or patient cooperation 3. If the target area is superficial, it is often useful to create your own acoustic window. The usual way to do this is with a stand-off pad. A water filled latex glove, jellied up on both sides will work, but there are other tricks as well. 4. Water immersion of a hand, foot or other body part can enhance visualization of superficial structures. Simply float the ultrasound probe in the water a few centimeters above the target structure. On your ultrasound screen, the acoustic layer of water will appear as a dark, anechoic line in the nearfield. The target structure will appear just farfield to this anechoic line. 5. Scan superficial structures with the 7.5 to 10 MHz linear array transducer. 6. Skeletal muscle will appear hypoechoic with interwoven echogenic striations and hyperechoic fascial planes. Adjacent tendons will appear brightly hyperechoic with visible linear fibers on long-axis scanning. 7. Any hypoechoic or anechoic interruption in the hyperechoic tendon fibers should raise the suspicion of a tendon disruption. Hypoechoic or anechoic areas may represent blood or, in subacute injuries, granulation tissue, where the tendon fibers have torn apart. 8. Subtle tendon damage, without actual tearing of the tendon fibers, may display an increase in the tendon cross-sectional area due to localized edema. Compare the area of interest to adjacent segments. 9. If the ultrasound beam is not aimed directly parallel to the tendon fibers, a false hypoechogenicity artifact may be noted (anisotropy).
| | |