Initial Evaluation
Check: 3 branches of Trigeminal, EOM, Bones, Teeth
Injuries to cheek between tragus and midcheek have injured parotid or facial nerve until proven otherwise
3 Questions
1. How is your vision (inquire about bilateral diplopia, unilateral, usually from cornea/lens)
2. Is your face numb
3. Are your teeth meeting normally
Test muscles of facial expression
Feel entire face, especially infraorbital rim, zygomatic frontal-junction (lateral portion of orbit.)
Pull on upper palate for Lefort. Palpate zygoma inside bucal mucosa
X-Rays
Waters View-orbital rims, infraorbital floor, maxilla, and maxillary sinuses
For mid-facial fractures, one view 30-degree occipitomental (Waters) is sufficient, do not need 3 view series. If positive, get CT scan. (J Trauma 52:688 2002)
Jug Handle-zygomatic arches and skull base
Caldwell-AP for frontal bones and sinuses
Normal series is Waters, Caldwell, and lateral
Extra-Townes for the zygoma and mandibular rami or
Panorex for mandibular condyles or base of skull


- Orbital outline
- Sinus outline
- Elephants trunk (as it looks like one) made up of zygomatic line laterally, which extends along the superior margin of the zygomatic arch and body, and the maxillary line medially, which extends along the inferior margin of the arch, body, and buttress of the zygoma and along the lateral wall of the maxillary sinus.
- Coronoid processthe tip of which should be equidistant from maxillary line on each side.
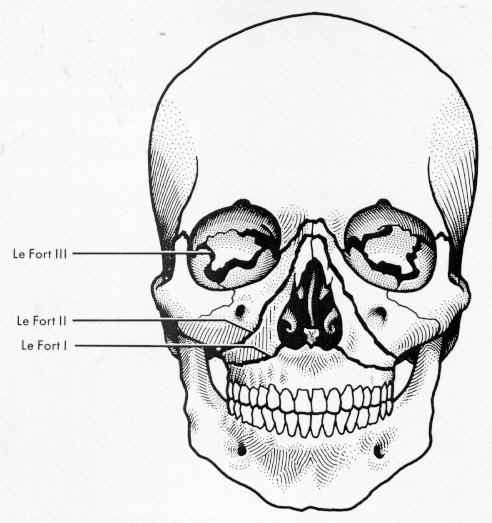
Maxillary Fractures
Lefort I-Maxilla and palate
II-Above and nasal pyramid
III-Above and severe craniofacial
Zygomatic Fracture
Get waters view, can be safely discharged
Tripod Fractures (Zygomaticomaxillary complex)
Eye will be pulled down, needs OMF surgery consult, admit for reduction
Orbital Floor Fx
blowout fx, herniation of orbit into maxillary sinus
observe eye for enophthalmos, sunken globe, or proptosis
Check EOM
To differentiate between muscular damage and true entrapment, do duction test. Anesthetize eye, then push sclera upwards to see if you can move eye
Test sensation over maxillary lip and teeth
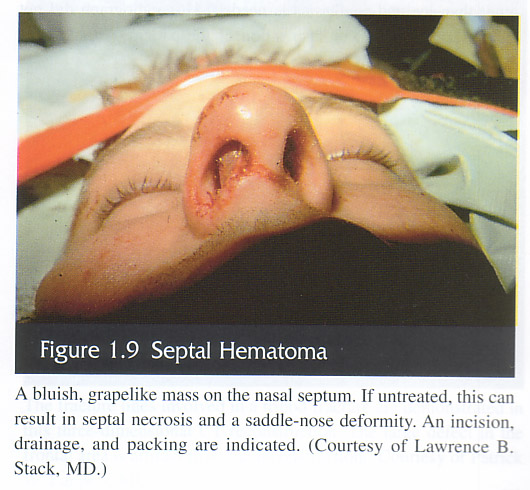
Nasal Fx
Palpate nasal bridge
Drain Septal hematomas Incise along inferior aspect after anesthesia
Mandibular Fx
Inspect floor of mouth for ecchymoses or hematoma, if present get CT c neg x-rays
Tongue blade test-if you can break the blade no mandible fracture. Palpate the mandibular condyles by palpating c finger in external auditory canal
Validation study showed 95% sens (The Journal of Emergency Medicine Volume 45, Issue 1, July 2013, Pages 8–12)
TMJ Dislocation
to reduce push down on third molars, then push slightly posterior
Dental Fxs and Avulsions
Ellis I-enamel, II-dentin, III-pulp, IV-Ridge
Frontal Bone or Sinus Fx
Forehead sensation
Ocular exam
If depressed, open or c posterior table involvement get ENT or Neurosurgery consultation
Naso-ethmoid-orbital (NEO) Injuries
High energy blows to bridge of nose
Pain with EOM or epiphora
Measure distances between medial canthi, normal is 35 to 40 mm. Any increase (telecanthus) appears as flattened nasal bridge. Increase in interpupillary distance (hypertelorism) signifies orbital fractures
Tenderness over medial canthi, perform the intranasal palpation test. Anesthetize nasal passage on side of injury insert hemostat into the nari and press laterally along the medial orbital rim while simultaneously palpating the medial canthus. Movement of the bone=NEO injury
Need facial CT
Need OMF surgical evaluation and abx
The solution to any facial bleeding should be angio, not surgery
First pack then go to the rads department
Review Article (Injury 1998;29(4):253-256)
origin of bleeding is often the internal maxillary artery and especially its intraosseous branches
brances of the internal carotid artery such as the lacrimal, zygomatic, as well as the anterior and posterior ethmoidal arteries
angiography can be very helpful, though there are “dangerous” arteries–vessels which contact the external and internal circulation
temporary reduction of the fractures will go a long way to stopping the bleeding
The American Journal of Emergency Medicine Volume 25, Issue 8, October 2007, Pages 988.e1-988.e5 Result list | previous < 35 of 35 > next SummaryPlus Full Text + Links PDF (199 K) View thumbnail images | View full size images Add to my quick links Cited by E-mail article Save as citation alert Export citation + link Set up a citation RSS feed (Opens new window) Related Articles in ScienceDirect Traumatic aneurysm of the maxillary artery: the role of… International Journal of Oral and Maxillofacial Surgery Close You are entitled to access the full text of this document Traumatic aneurysm of the maxillary artery: the role of interventional radiology International Journal of Oral and Maxillofacial Surgery, Volume 24, Issue 5, October 1995, Pages 336-339 S.N. Rogers, M. Patel, J.C. Beirne and T.E. Nixon Abstract Two cases of post-traumatic aneurysm of the maxillary artery are described. The first patient was a 20-year-old man who sustained a Le Fort III type fracture in a road traffic accident. He experienced two episodes of significant maxillofacial haemorrhage, the first following admission and the second 5 days after initial reduction and fixation of his midfacial fractures. The second patient was a 23-year-old man with a bilateral cleft palate and extreme midfacial hypoplasia who underwent Le Fort I osteotomy. Significant bleeding commenced 3 h postoperatively and was not completely controlled by anterior and posterior nasal packing. Both the aneurysms were diagnosed on selective carotid angiography and successfully treated by embolization. Abstract | Abstract + References | PDF (2706 K) Pseudoaneurysm of internal maxillary artery secondary t… Journal of Oral and Maxillofacial Surgery Close You are entitled to access the full text of this document Pseudoaneurysm of internal maxillary artery secondary to gunshot wound managed by endovascular technique Journal of Oral and Maxillofacial Surgery, Volume 62, Issue 4, April 2004, Pages 500-502 Deepak G. Krishnan, Amir Marashi and Anil Malik SummaryPlus | Full Text + Links | PDF (254 K) Life-threatening complications and irreversible damage … Injury Close You are entitled to access the full text of this document Life-threatening complications and irreversible damage following maxillofacial trauma Injury, Volume 29, Issue 4, May 1998, Pages 253-256 L. Ardekian, D. Rosen, Y. Klein, M. Peled, M. Michaelson and D. Laufer Abstract Trauma remains one of the principal causes of mortality in the western world, especially among young adults. The most serious immediate life-threatening complication following maxillofacial trauma is airway obstruction. The onset can be sudden, as with foreign body aspiration, or following soft-tissue damage that can lead at a later stage to airway-compromising oedema. The medical literature regarding facial trauma appears to support the hypothesis that maxillofacial trauma alone is rarely life threatening, or will not lead to life-threatening conditions unless associated with airway compromise. There are some causes of life-threatening complications following trauma to the maxillofacial region such as massive bleeding or undiagnosed cervical spine injury. However, there are some situations that may cause irreversible damage unless immediate operation is undertaken. The almost complete lack of reports dealing with death or irreversible damage in trauma involving the maxillofacial region prompted us to review and analyse the importance of immediate intervention following trauma to the maxillofacial region, in order to treat life-threatening complications and prevent irreversible damage. Abstract | Abstract + References | PDF (537 K) Transarterial embolization in the treatment of life-thr… The American Journal of Emergency Medicine Close You are entitled to access the full text of this document Transarterial embolization in the treatment of life-threatening maxillofacial bleeding The American Journal of Emergency Medicine, Volume 20, Issue 4, July 2002, Pages 380-381 Chih-Yuan Lee, Ming-Hong Chen, Tzu-Hsin Lin and Shyr-Chyr Chen PDF (1435 K) Successful hemostasis of intractable nasal bleeding wit… Otolaryngology – Head and Neck Surgery Close You are entitled to access the full text of this document Successful hemostasis of intractable nasal bleeding with a Sengstaken-Blakemore tube Otolaryngology – Head and Neck Surgery, Volume 134, Issue 6, June 2006, Pages 1053-1054 Seiji Morita, Masayoshi Shibata, Yoshihide Nakagawa, Isotoshi Yamamoto and Sadaki Inokuchi SummaryPlus | Full Text + Links | PDF (550 K) View More Related Articles doi:10.1016/j.ajem.2007.02.039 How to Cite or Link Using DOI (Opens New Window) Copyright © 2007 Elsevier Inc. All rights reserved. Case Report Angioembolization as an effective alternative for hemostasis in intractable life-threatening maxillofacial trauma hemorrhage: case study Shih-Chi Wua, b, E-mail The Corresponding Author, Ray-Jade Chenb, E-mail The Corresponding Author, Kwo-Whei Leec, E-mail The Corresponding Author, Cheng-Cheng Tunga, E-mail The Corresponding Author, Wen-Pei Lina, E-mail The Corresponding Author and Poon Yia, E-mail The Corresponding Author aDivision of Trauma, Changhua Christian Hospital, Changhua, 500 Taiwan, ROC bTrauma and Emergency Center, China Medical University Hospital, Taichung 404, Taiwan, ROC cDivision of Radiology, Changhua Christian Hospital, Changhua, 500 Taiwan, ROC Available online 5 October 2007. Article Outline References Life-threatening maxillofacial trauma hemorrhage is not common; oronasal hemorrhage from maxillofacial trauma can often be managed with manual compression or efficient tight packing. Surgery is reserved for cases where failure of tight packing occurs. However, the use of angioembolization might decrease the need for blood transfusion and provide an effective alternative for early hemostasis after packing failure. We report 7 cases wherein angioembolization was successfully performed for hemostasis of life-threatening maxillofacial trauma hemorrhage. Maxillofacial injuries often result in airway compromise, hemorrhage, and bony fracture [1], [2] and [3]. As the popularity of restraint-equipped automobiles and airbags expanded, reports of maxillofacial injuries with airbag deployment increased [4] and [5]. Most hemorrhages from maxillofacial injuries can be managed with adequate nasal packing or direct pressure or even wiring of mandibular fractures [6]. However, persistent life-threatening hemorrhage is not common, the incidence rate ranges from 1.2% to 4.5% in maxillofacial injuries [1], [2], [3] and [6]. Nonetheless, if persistent life-threatening hemorrhage occurs, emergent life-saving surgery with open reduction and internal fixation or ligation of focal vessels (eg, internal maxillary artery, external carotid artery) might be necessary [6] and [7]. On the other hand, transcatheter arterial embolization (TAE) has been applied in the management of intractable posterior epistaxis and has achieved a high success rate with a low complication rate [8], [9] and [10]. Therefore, it was also considered as an alternative in the management of intractable hemorrhage in life-threatening maxillofacial trauma [3], [11] and [12]. Herein, we report 7 cases where angioembolization was successfully performed in hemostasis of life-threatening maxillofacial trauma hemorrhage. Among 7 patients with life-threatening maxillofacial hemorrhage, we present 2 selected patients for discussion due to exemplary, vigorous hemorrhage. The maxillofacial computed tomography (CT) scans were obtained using a GE Light Speed Scanner (GE Medical Systems, Milwaukee, Wis). Patients received 100 mL of intravenous bolus of nonionic contrast Ioversol (Optiray, Mallinckrodt Inc, Hazelwood, Mo). Ten-millimeter cuts were obtained. All CT scans were initially read by staff trauma surgeons and are later reviewed by staff radiologists. Contrast extravasation/contrast blush is defined as a focus of high-attenuation contrast material on CT film. The angioembolization was performed by interventional radiologists. Arterial access was obtained via right femoral artery, and a 6 Fr# right femoral sheath was used. A 5 Fr# RC1 catheter (Cook, Bloomington, Indiana) was used for external carotid artery catheter. Patients underwent embolization with coils (Cook, Bloomington, Indiana or Boston, Scientific, Watertown, Mass) and/or Gelfoam (Pharmacia, Kalamazoo, Mich). A 19-year-old back-seated male passenger was ejected from a vehicle after a crash and was sent to our emergency department (ED) for resuscitation where management followed the guidelines of Advanced Trauma Life Support. The patient’s blood pressure was 140/80 mm Hg, and heart rate 120 beats/min on arrival. Emergent x-rays showed left zygomatic and orbital bony fracture, and a helical CT revealed severe brain contusion with swelling and grade III liver injury. However, vigorous active bleeding from the nares and oral cavity was noted. The patient initially received direct pressure tight nasal packing, which failed. Persistent hemorrhage would result in hypovolemic shock if the bleeder was not arrested; therefore, an emergent angiography via the femoral route was performed, which showed contrast extravasation of the left maxillary artery (Fig. 1A). Embolization of the left maxillary artery was performed with 2 microcoils. A follow-up external carotid artery angiogram showed that the bleeder had been embolized (Fig. 1B), and thus, no further oronasal bleeding was detected. The patient was subsequently admitted to our intensive care unit for further observation; however, on the sixth day, the patient died as a result of severe brain injury. Image Display Full Size version of this image (159K) Fig. 1. A, Angiography shows left maxillary artery (large arrow) and active contrast blush (small arrow). B, No more contrast blush after coil embolization (small arrow). C, Right distal internal maxillary artery (large arrow) active contrast blush and traumatic pseudoaneurysm formation (small arrow). D, Right distal internal maxillary artery pseudoaneurysm was occluded after coil embolization (small arrow). A 39-year-old male patient had a motorcycle accident and was sent to the ED. On arrival, the patient’s blood pressure was 70/40 mm Hg, heart rate 145 beats/min; he received vigorous resuscitation and became hemodynamically stable. X-rays showed frontal bone fracture and right fourth to sixth rib fracture with a hemothorax. Helical CT revealed intracranial and subarachnoid hemorrhage and a grade III liver injury without contrast blush. After hemodynamics were stabilized, the patient was admitted to our emergency intensive care unit for further observation. However, sudden onset of vigorous hemorrhage from the nares and oral cavity were noted on day 10, and tight packing and compression were performed but failed and persistent hemorrhage may induce hypovolemic shock. An emergent carotid artery angiography via the femoral route showed right distal internal maxillary artery active contrast leakage and traumatic pseudoaneurysm formation (Fig. 1C). Coil embolization of the distal main trunk of the right internal maxillary artery occluded the pseudoaneurysm (Fig. 1D), and no further oronasal bleeding was detected. However, the patient underwent laparoscopic left lung wedge resection due to iatrogenic lung injury and hemorrhage after removal of the chest tube on the 20th day. The patient was discharged after careful management, and no facial numbness or tissue necrosis or other symptoms were noted during outpatient follow-up. The characteristics of the 7 patients are listed in Table 1. The mean age of all subjects (6 males and 1 female) was 32.9 ± 14.1 years. The mean injury severity score was 41.7 ± 13.6, and all patients had blunt injuries. Time to embolization after injury and the amount of blood transfused after embolization are shown in Table 2. The average time to embolization was 11.6 ± 7.3 hours. Four patients (57.1%) died of associated severe brain injury in spite of arresting maxillofacial hemorrhage. Additional blood transfusions were not required after facial TAE in all patients; however, some patients received a blood transfusion due to other sources of hemorrhage (Table 2). There were 3 survivors, 1 patient (patient 2) with persistent hemorrhage after failure of tight nasal packing for 19 hours, who received successful angioembolization. The remaining 2 patients (patients 6 and 7) experienced delayed oronasal bleeding 10 and 11 days after the initial crash, and angioembolization was performed after failure of attempting hemostasis with tight nasal packing. There were no stroke, facial numbness, tissue necrosis, or other symptoms that occurred in these 3 survivors during outpatient follow-up. Table 1. Characteristics of maxillofacial injuries Patient Age/Sex Injury mechanism Injury type ISS Vessel injured and embolized Head injuries Lefort injury Associated injuries 1 19/male Blunt (MVC) Brain contusion Lefort II Liver grade III injury 35 Left maxillary artery 2 22/male Blunt (MCC) ICH, Liver grade IV injury 48 Bilateral lingual artery, perigingival branch Skull bone fracture Lung injury 3 22/male Blunt (crush) Skull bone fracture Lefort II 26 Right accessory maxillary artery 4 55/male Blunt (fall) ICH Pelvic fracture 59 Right maxillary artery Skull bone fracture 5 26/female Blunt (MCC) Skull bone fracture, SAH Lefort II Liver grade V injury 57 Right facial artery, mandibular branch 6 39/male Blunt (MCC) ICH, SAH Lefort II Right hemothorax 50 Right distal internal maxillary artery Liver grade III injury 7 47/male Blunt (MCC) EDH Lefort II 29 Right distal internal maxillary artery, sphenopalatine branch MVC indicates motor vehicle crash; MCC, motorcycle crash; ISS, injury severity score; ICH, intracranial hemorrhage; SAH, subarachnoid hemorrhage; EDH, epidural hemorrhage. Table 2. Time to embolization after injury and amount of blood transfused post procedure Patient no. Time to TAE after injury or delayed bleeding (h) BT before TAE (mL) BT after TAE (mL) Local effect Systemic effect and outcome 1 17.7 2000 0 No more nasal bleeding after facial TAE Die of brain injury 2 19.2 1500 500 No further nasal bleeding after facial TAE Delayed liver hemorrhage on the 12th day, received BT and liver TAE Survived 3 5.8 2000 250 No further nasal bleeding after facial TAE Died of brain injury 4 4.0 1500 2000 No further nasal bleeding after facial TAE Died of brain injury Associated pelvic fracture with bleeding, received BT and pelvic TAE 5 2.0 1000 12,000 No further nasal bleeding after facial TAE Died of brain injury and severe liver injury induced hemorrhagic shock 6 17.0 5500 0 No further nasal bleeding after facial TAE Iatrogenic lung injury and bleeding on the 20th day after removing chest tube, received laparoscopic thoractomy, BT 1500 mL Small groin hematoma Survived 7 15.2 1500 0 No further nasal bleeding after facial TAE Survived BT indicates blood transfusion. Life-threatening maxillofacial trauma bleeding is not common, the incidence rate ranges from 1.2% to 4.5% in maxillofacial injuries [1], [2], [3] and [6], which often results in airway compromise or hypovolemia [1], [2] and [3]. Management should follow the guidelines of Advanced Trauma Life Support with protection of the airway being the first priority [13]. Oronasal hemorrhage from venous origin or minor arterial vessels due to maxillofacial trauma can often be managed efficiently with manual compression or tight packing [3] and [6]. Some cases with serious maxillofacial trauma hemorrhage can result in hemorrhagic shock and can often require emergent open reduction and internal fixation for hemostasis [1] and [6]. Occasionally, complicated techniques with ligation of focal vessels (eg, internal maxillary artery, external carotid artery) are necessary for arresting hemorrhage [7], however, this manipulation procedure could be laborious and might impinge on the stability of the cervical spine and may cause further damage. An alternative method for controlling hemorrhage is TAE [3], [11], [12] and [14], which has been widely used in severe nontraumatic epistaxis for many years [9] and [10]. Although the wide application of TAE in traumatic torso or intra-abdominal solid organ hemorrhage or pelvic fracture had been reported [15], knowledge of TAE usage for maxillofacial hemorrhage was mostly gained from otolaryngology literature concerning patients with severe epistaxis [8], [9] and [10]. However, TAE has been recently reported as the primary choice for life-threatening maxillofacial trauma bleeding [2], [3], [11] and [12]. In this series, 7 patients experienced life-threatening maxillofacial trauma hemorrhage and received TAE; no further nasal bleeding were detected after the procedure. Additional blood transfusions were necessary in 4 patients due to other sources of hemorrhage (Table 2). Four patients died of brain injuries. No facial numbness, tissue necrosis, or other symptoms were detected in the 3 survivors during outpatient follow-up. Arresting nasal hemorrhage shows that TAE may serve as an efficient alternative for hemostasis in life-threatening maxillofacial hemorrhage. Associated cerebral trauma and severe brain injuries are common in maxillofacial trauma. To our knowledge, persistent maxillofacial hemorrhage might result in brain hypoperfusion as well as secondary brain injuries, which often result in adverse outcomes [16] and [17]. However, it has been reported that early treatment of cerebral hypoperfusion status may reduce secondary brain injury and decrease mortality [18]. We believe that in cases where failure of tight packing occurs, early hemostasis for maxillofacial hemorrhage with TAE might be helpful in shortening the hypoperfusion status and preventing the brain from further damage. Additional blood transfusions were not required after facial TAE in all patients; however, some patients received a blood transfusion due to other sources of hemorrhage (Table 2). The decreased amount of blood transfusion was inclined to reduce the possibilities of blood-borne diseases [19]. In our series, there were no stroke, facial numbness, tissue necrosis, or other symptoms that occurred in the 3 survivors. Although angioembolization is quite safe for hemorrhage from branches of external carotid artery, it is not without hazard when embolizing internal maxillary artery. The possibilities of embolus migrating into the brain and causing cerebrovascular accident or stroke should be noted. However, the reported risk of dislodging the embolizing agent is about 1.9% in experienced hands [20]. The oronasal status of patients 6 and 7 were normal initially; however, both patients experienced delayed oronasal bleeding 10 and 11 days after the initial crash. Tight packing of the nares was performed but failed; thus, embolization was performed within 24 hours, and the bleeding was stopped. Although the exact reason for the delayed hemorrhage is unclear, as we know, a higher injury severity score often predicts nonoperative management failure in blunt splenic injuries [21], it is to be elucidated whether a higher injury severity score is of predictive value in delayed maxillofacial hemorrhage. On the other hand, there were organized thrombus and blood clots after vessel injuries in normal subjects [22] and [23]. In this series, both patients were with severe head and brain injuries (head abbreviated injury score = 5) (Table 1) and were under bedridden resting state within the first week of hospital stay. It is of interest whether regaining activities after recovery might result in breakdown of the stabilized blood clots and induce delayed hemorrhage. However, possibilities of delayed life-threatening hemorrhage after maxillofacial trauma should be considered. Life-threatening maxillofacial trauma hemorrhage is not common; the oronasal hemorrhage from maxillofacial trauma can often be managed with manual compression or efficient tight packing. Emergency surgery is reserved for cases where failure of tight packing occurs. In this series, TAE decreases the need for blood transfusion and provides an effective alternative for early hemostasis after packing failure, which might shorten hypoperfusion status and prevent secondary brain injury. However, the possibilities of delayed life-threatening maxillofacial hemorrhage have to be considered, and we suggest transarterial embolization to be considered as the primary choice of treatment. Further prospective studies elucidating the role of early transarterial embolization in life-threatening maxillofacial trauma hemorrhage and determining the relationship between higher injury severity score and delayed maxillofacial hemorrhage are necessary.
References [1] T.C. Tung, W.S. Tseng and C.T. Chenet al., Acute life-threatening injuries in facial fracture patients: a review of 1025 patients, J Trauma 49 (3) (2000), pp. 420424. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (12) [2] W.G. Yang, T.R. Tsai and C.C. Hung et al., Life-threatening bleeding in facial fracture, Ann Plast Surg 46 (2) (2001), pp. 159162. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (4) [3] R.P. Bynoe, A.J. Kerwin and H.H. Parker III et al., Maxillofacial injuries and life-threatening hemorrhage: treatment with transcatheter arterial embolization, J Trauma 55 (1) (2003), pp. 7479. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (6) [4] C. Brookes, S. Wang and J. McWilliams, Maxillofacial injuries in North American vehicle crashes, Eur J Emerg Med 10 (1) (2003), pp. 3034. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (4) [5] R.X. Murphy Jr, K.L. Birmingham and W.J. Okunski et al., The influence of airbag and restraining devices on the patterns of facial trauma in motor vehicle collisions, Plast Reconstr Surg 105 (2) (2000), pp. 516520. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (20) [6] L. Ardekian, N. Samet and Y. Shoshani et al., Life-threatening bleeding following maxillofacial trauma, J Craniomaxillofac Surg 21 (8) (1993), pp. 336338. Abstract | PDF (573 K) | View Record in Scopus | Cited By in Scopus (14) [7] M.M. Cullen and T.A. Tami, Comparison of internal maxillary artery ligation versus embolization for refractory posterior epistaxis, Otolaryngol Head Neck Surg 118 (5) (1998), pp. 636642. SummaryPlus | Full Text + Links | PDF (62 K) | View Record in Scopus | Cited By in Scopus (33) [8] N.P. Christensen, D.S. Smith and S.L. Barnwell et al., Arterial embolization in the management of posterior epistaxis, Otolaryngol Head Neck Surg 133 (5) (2005), pp. 748753. SummaryPlus | Full Text + Links | PDF (291 K) | View Record in Scopus | Cited By in Scopus (4) [9] G. Ricci, E. Molini and M. Hamam et al., Treatment of severe epistaxis by superselective embolization: a review of 22 cases, Rev Laryngol Otol Rhinol (Bord) 125 (4) (2004), pp. 247251. View Record in Scopus | Cited By in Scopus (1) [10] J. Nickel, W. Sachs and R. Andresen, Selective embolisation of posttraumatic intractable epistaxis, Rontgenpraxis 55 (2) (2003), pp. 7277. View Record in Scopus | Cited By in Scopus (0) [11] Z.H. Baqain, C. Thakkar and N. Kalavrezos, Superselective embolization for control of facial haemorrhage, Injury 35 (4) (2004), pp. 435438. SummaryPlus | Full Text + Links | PDF (261 K) | View Record in Scopus | Cited By in Scopus (0) [12] P. Siritongtaworn, Management of life-threatening hemorrhage from facial fracture, J Med Assoc Thai 88 (3) (2005), pp. 382385. View Record in Scopus | Cited By in Scopus (1) [13] American College of Surgeons, Committee on Trauma, Advanced trauma life support manual (7th ed.), American College of Surgeons, Chicago (Ill) (2004). [14] R. Murakami, T. Kumazaki and H. Tajima et al., Transcatheter arterial embolization as treatment for life-threatening maxillofacial injury, Radiat Med 14 (4) (1996), pp. 197199. View Record in Scopus | Cited By in Scopus (2) [15] G.C. Velmahos, K.G. Toutouzas and P. Vassiliu et al., A prospective study on the safety and efficacy of angiographic embolization for pelvic fracture and visceral injuries, J Trauma 53 (2) (2002), pp. 303308. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (58) [16] R. Hlatky, C.F. Contant and P. Diaz-Marchan et al., Significance of a reduced cerebral blood flow during the first 12 hours after traumatic brain injury, Neurocrit Care 1 (1) (2004), pp. 6983. [17] E. Jeremitsky, L. Omert and C.M. Dunham et al., Harbingers of poor outcome the day after severe brain injury: hypothermia, hypoxia, and hypoperfusion, J Trauma 54 (2) (2003), pp. 312319. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (39) [18] J. Ghajar, Traumatic brain injury, Lancet 356 (9233) (2000), pp. 923929. SummaryPlus | Full Text + Links | PDF (120 K) | View Record in Scopus | Cited By in Scopus (70) [19] M.E. Chamberland, Surveillance for bloodborne infections, Thromb Haemost 82 (2) (1999), pp. 494499. View Record in Scopus | Cited By in Scopus (8) [20] L. Remonda, G. Schroth and M. Caversaccio et al., Endovascular treatment of acute and subacute hemorrhage in the head and neck, Arch Otolaryngol Head Neck Surg 126 (10) (2000), pp. 12551262. View Record in Scopus | Cited By in Scopus (19) [21] L.K. McIntyre, M. Schiff and G.J. Jurkovich, Failure of nonoperative management of splenic injuries: cause and consequences, Arch Surg 140 (6) (2005), pp. 563568. [22] K. Jurk and B.E. Kehrel, Platelets: physiology and biochemistry, Semin Thromb Hemost 31 (4) (2005), pp. 381392. Full Text via CrossRef [23] J.M. Stassen, J. Arnout and H. Deckmyn, The hemostatic system, Curr Med Chem 11 (17) (2004), pp. 22452260. View Record in Scopus | Cited By in Scopus (22)
Solution to midface bleeding-McKesson Prop
| | |