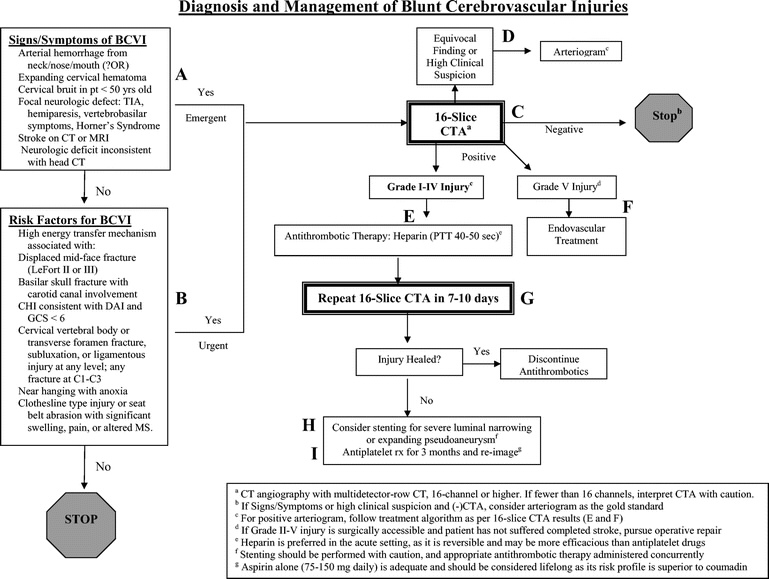
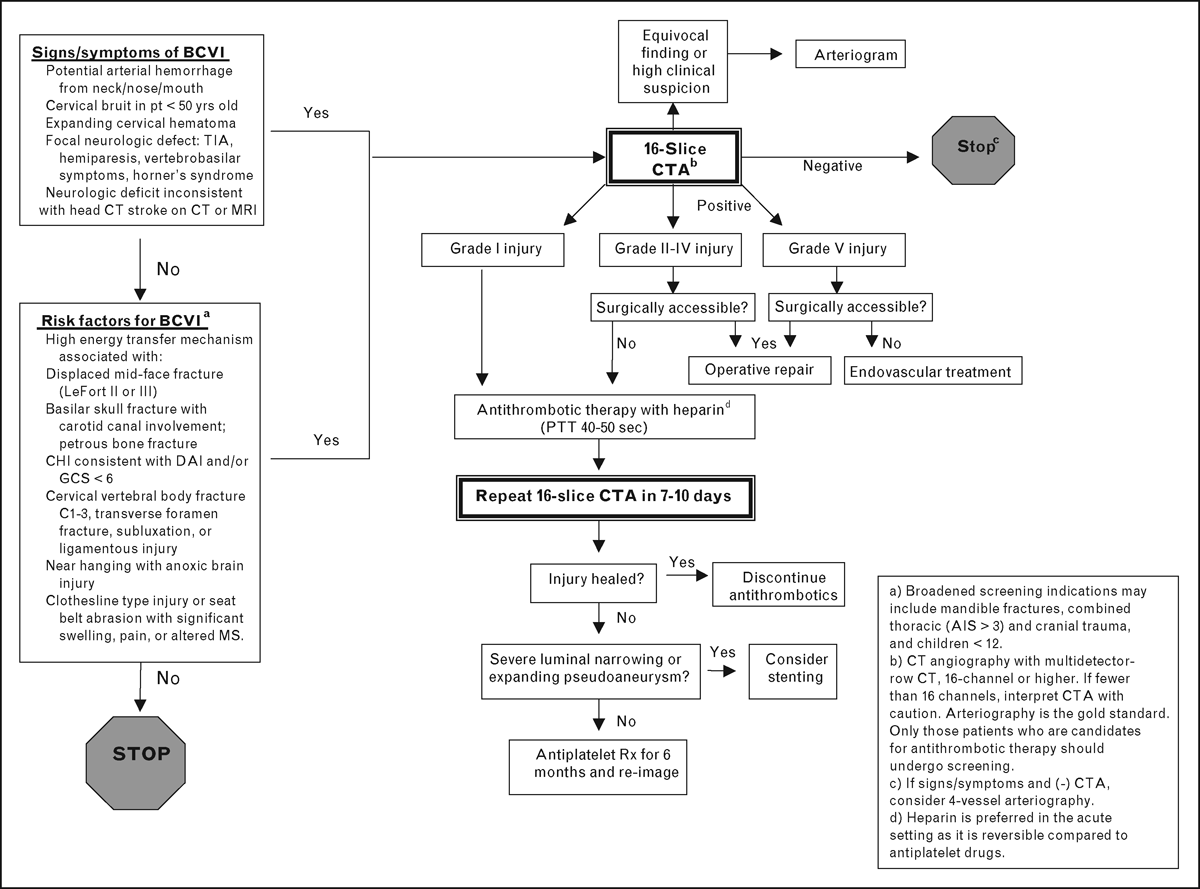
Screen basilar skull fx, c-spine fx, facial fx, gcs < 8, lateralizing facial neurodeficits
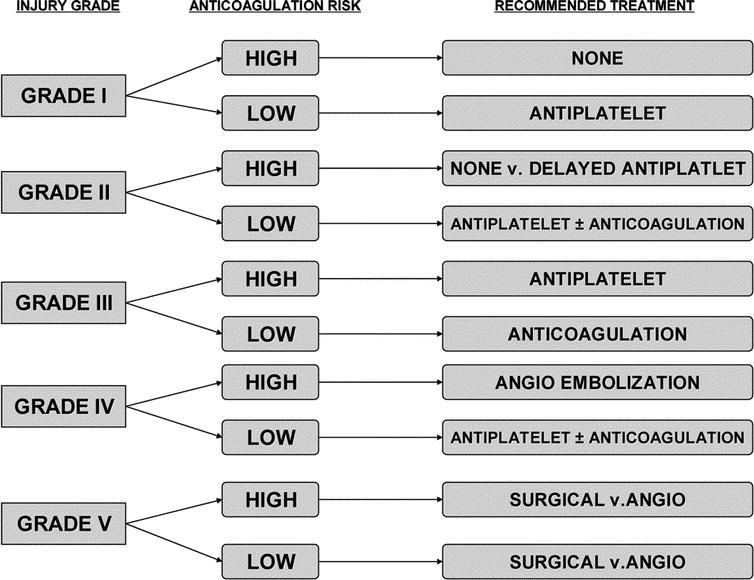
Antiplatelet both vertebral and carotid injuries
Other Injuries Associated with Cervical Spine Trauma
Vertebral artery injury This injury is seen in up to 11% of cervical blunt trauma populations and presents as an expanding cervical hematoma, a bruit in patients under 50 years of age, an infarct seen on CT, significant facial hemorrhage from ears, nose or face, or symptoms consistent with a posterior circulation stroke (13, 14). In such patients, MRA or angiography is recommended to evaluate the possibility of vertebral artery injury (VAI). Patients with vertebral subluxation, facet dislocations, or foramen transversarium fractures are at increased risk for VAI and probably should undergo imaging studies as well (15). Injury types are shown in table I. Symptoms of VAI reflect a posterior circulation stroke and range from ataxia, vertigo, or blindness, to focal deficits or complete cord injury. Treatment options are observation versus heparin. Regardless of the type of injury (except grade V), heparin has been shown to be of modest benefit in symptomatic patients (14). Due to the risk of anticoagulation in the blunt trauma patient, it should only be considered in conjunction with neurosurgery and trauma surgery consultation.
Table I: Grading of VAI (I) Dissection < 25% (II) Dissection > 25% (III) Pseudo-aneurysm (IV) Complete arterial occlusion (V) Transection
Landmark Article: Annals of Surgery Volume 223(5) May 1996 pp 513-525 Blunt Carotid Injury: Importance of Early Diagnosis and Anticoagulant Fabian, Timothy
Most common sites of injury
Carotid 2 cm distal to bifurcation
Vertebral between C2 and the skull base
Dissection of the internal carotid artery is the creation of a channel within the wall of the vessel resulting from disruption of the intima. It is manifested angiographically by 1. a narrowing of the “true” lumen flow of blood throug a disrupted intima associated with 2. a linear lucent line representing the intima/media component that has been dissected by the “intramural” hematoma.Dissection in normal healthy vessels is uncommonly seen. it is far more likely to result from vessels with medial degeneration. I have seen three unquestionable dissections after trauma proven by angiography. Two were blunt, an abdominal aortic injury, and a subclavian artery injury. Both were in elderly men. The third was a young man who sustained a gunshot wound of the axillary artery. This was proven to be a dissection when the guidewire entered the false lumen. The imaging appearance of dissections is much more readily evident on MR and CTA because those cross sectional imaging techniques allow us to see the soft tissue of the wall. It is possible to identify dissections as high attenuation signals (representing clotted hematoma) on CT within the wall. MR can also delineate such wall abnormalites. Angiographic diagnosis of ICA “dissections” is most difficult because many injuries of the ICA, especially intimal trauma, result in spasm which can resemble a dissected vessel. Thrombosis will also give such an appearance that is presumed to be a dissection. but that is unproven. . intimal flaps, which are represented as short linear radiolucencies in the contrast column, are a much more common sequellae of trauma and are often erroneously labeled as dissections by BOTH SURGEONS AND RADIOLOGISTS.
Others say evaluation for this injury is futile 11 in 35212 had a stroke (Arch Surg 2004;139:609)
Largest series on parameters of multislice CT SENS 97.7 SPEC 100% (J Trauma 2006;60:925)
CTA screening protocol (J Trauma 2009;67(3):551)
they used modified Denver Criteria
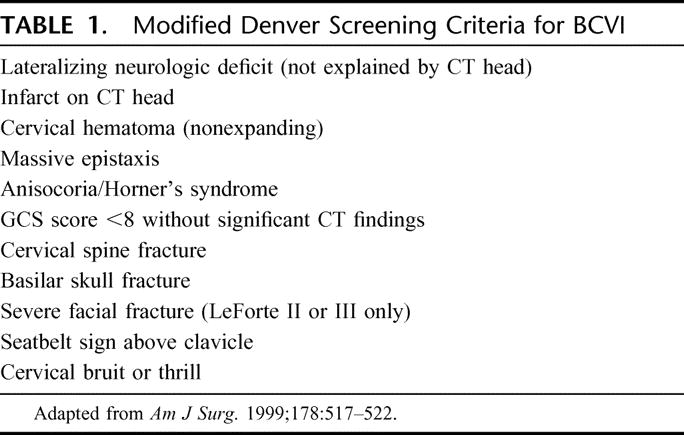
New Improved Screening Criteria from Fabian’s Group (J Trauma 2011;70:1058)
- CTA seems unreliable
- Skull Base Fractures
- Horner’s
- C-Spine Fx
- Lefort II or III
- Soft Tissue Neck Injuries
- Neuro findings inconsistent with radiology
Data may favor early treatment of concomitant BCVI with intracranial hemorrhage (The Journal of Trauma and Acute Care SurgeryIssue: Volume 72(2), February 2012, p 338–346)
Updated screening study shows a significant number of patients suffering BCVI are not captured by current screening guidelines. Screening for BCVI should be considered in patients with
- mandible fractures
- complex skull fractures
- traumatic brain injury with thoracic injuries
- scalp degloving
- thoracic vascular injuries.
(J Trauma Volume 72(2), February 2012, p 330–337)
Aspirin Seems as Good as Anticoagulation
antiplatelet treatment compared with anticoagulation treatment for cervical artery dissection (CADISS): a randomised trial The CADISS trial investigators †Listed at the end of the article Published Online: 12 February 2015 Open Access Article has an altmetric score of 67 DOI: http://dx.doi.org/10.1016/S1474-4422(15)70018-9