DPA
Percutaneous DPA is the foster child of DPL (Int J of Surg 2007;5:167)
One of the original articles on closed dpl
showed that FAST may be inaccurate even in hypotensive patients when performed by surgeons (Article)
One of the original trials showing the safety of closed for DPL or DPA
DPL
MA of open vs. closed (J Trauma 48(6):1091)
closed needed more conversions to open-duh, but closed is much quicker. complication rates similar
- A 2500 patient study also showed no difference in complications (Injury, Int. J. Care Injured 31 (2000) 479)
J Trauma. 1985 Mar;25(3):228-31. Related Articles, LinksUse of peritoneal lavage to evaluate abdominal penetration. Merlotti GJ, Marcet E, Sheaff CM, Dunn R, Barrett JA. A retrospective study was undertaken to evaluate peritoneal lavage in detecting abdominal penetration. Two hundred thirty-five patients with thoracoabdominal, flank, or tangential abdominal gunshot wounds were lavaged. Of these patients, 44 (18.7%) had positive lavages, defined as red blood cell counts greater than 10,000 cells/mm3, white blood cell counts greater than 500 cells/mm3, or the presence of bile, feces, or vegetable matter. There were 13.6% false positives and 1.0% false negatives, with an overall accuracy of 96.6%. The results were unaffected by mechanism or site of injury. If the criteria were changed to include red blood cell counts greater than 100,000 cells/mm3, there would have been no false positives, but an unacceptably high 11.1% false negative rate. Therefore we conclude that peritoneal lavage can be a reliable indicator of abdominal penetration provided sufficiently sensitive criteria are used. These criteria should include red blood cell counts greater than 10,000 cells/mm3 instead of 100,000 cells/mm3.
Diagnostic peritoneal lavage through an abdominal stab wound (The American Journal of Emergency Medicine Volume 21, Issue 7 , November 2003, Pages 559-560)
1: J Trauma. 1988 Jan;28(1):17-23. Related Articles, LinksPeritoneal lavage in penetrating thoraco-abdominal trauma. Merlotti GJ, Dillon BC, Lange DA, Robin AP, Barrett JA. Trauma Unit, Cook County Hospital, Chicago, IL 60612. Forty-five consecutive patients with penetrating thoraco-abdominal trauma underwent surgical exploration to evaluate the ability of peritoneal lavage to detect peritoneal penetration. Eight patients fulfilled standard criteria for operation and did not undergo lavage. The remaining 37 patients underwent diagnostic peritoneal lavage using a closed technique before exploratory laparotomy. Using 10,000 RBC/mm3 as our previously established criterion for peritoneal penetration, there were seven true positive, one false positive, 28 true negative, and one false negative lavage for an overall accuracy of 94.6% with 87.5% sensitivity and 96.6% specificity as determined by subsequent laparotomy. While 33% of this patient cohort were found to have significant injuries (four had isolated diaphragmatic injuries, all detected by peritoneal lavage), 67% were subjected to negative surgical exploration, as accurately predicted by peritoneal lavage. Negative laparotomy carried a 10.7% operative morbidity. Based on these data we advocate diagnostic peritoneal lavage in patients with thoraco-abdominal penetrating trauma who otherwise lack operative indications.
J Trauma 2007;62:853 claim of no missed injuries at 100,000 if combined with WBC>500, presence of bile or amylase 23 hour obs for negatives
Where you will get burned:
Duodenum, Pancreas, Mesentery, and Hollow Viscous, diaphragm
local wound exploration for anterior abdominal stab wounds, triple contrast CT scan for flank, back, pelvic, and right-sided thoracoabdominal wounds, sigmoidoscopy / cystography if needed for pelvic area wounds, and laparoscopy or thoracoscopy for left-sided thoracoabdominal wounds (c.f. above).
DPL for abd stab wounds (J of Trauma 2001;51:939-943) If 10 cc of blood withdrawn, observe. If not then send. If WBC <500 per cc or RBC < 1000.
Any penetrating trauma deserves a triple contrast study (J Trauma 2001;51:860-869)
Ng, AKT, Simons, RK, Torreggiani, WC, et al. Intraabdominal Free Fluid Without Solid Organ Injury in Blunt Abdominal Trauma: An Indication for Laparotomy. J Trauma, 2002;52:11341140.
The evaluation of patients with blunt abdominal trauma has undergone significant evolution in the last twenty-five years. The standard in the past was the performance of diagnostic peritoneal lavage to determine if the patient had suffered injuries that required operative intervention. With the evolution of non-invasive techniques, abdominal ultrasound and computerized tomography have become the currently utilized methods to assess for intraabdominal injury. The purpose of the present study was to evaluate all patients who presented with blunt abdominal trauma to determine the incidence, significance, and implications of free fluid without solid organ injury found on abdominal US or CT. In the patient with solid organ injury, the presence of fluid on abdominal CT is thought to represent blood from the injured solid organ. Free fluid without solid organ injury may represent an undetected solid organ injury, bleeding from the mesentery which may or may not require operative intervention, or an otherwise unseen hollow viscus injury. The question arises: what should be done in patients whose CT demonstrates free fluid but no solid organ injury?
This first of two papers addressing this question was a retrospective study of all patients who presented with blunt abdominal trauma. The patients underwent abdominal sonography to determine the presence or absence of free fluid in the abdomen. Unstable patients with a positive abdominal ultrasound were taken to the operating room for exploratory laparotomy. Stable patients with a positive abdominal ultrasound underwent further diagnostic imaging using CT. Patients who had CT evidence of solid organ injury were excluded from the study, while those who had free intraabdominal fluid without identifiable solid organ injury to explain the presence of the free fluid were the subjects of this study. Twenty-eight patients who had free fluid without solid organ injury constituted the study group. Twelve of these underwent a therapeutic laparotomy, and 3 having a non-therapeutic laparotomy. Of the remainder who were observed, most of whom had only trace amounts of free fluid, only 1 subsequently required operative intervention. The authors conclude that laparotomy should be recommended for all patients with blunt abdominal trauma who have more than trace amounts of free fluid in the absence of solid organ injury. Of note, the clinical finding of seatbelt bruising together with free fluid should always be considered an indication for laparotomy, with the preoperative diagnosis of hollow viscous disruption.
Rodriguez, C, Barone, JE, Wilbanks, TO, et al. Isolated Free Fluid on Computed Tomographic Scan in Blunt Abdominal Trauma: A Systematic Review of Incidence and Management. J Trauma, 2002;53:7985.
The second paper concerning the significance of free fluid without solid organ injury comes to a different conclusion. The authors of the present paper systematically reviewed the recent literature in order to develop guidelines for the management of this problem. They found, unfortunately for us, that the literature is inconclusive. The incidence of non-therapeutic laparotomy in this setting was approximately 75%. These authors therefore do not recommend that a patient be rushed to the operating room. Instead, diagnostic peritoneal lavage and/or observation with serial physical examinations are two acceptable strategies. The authors offer an algorithm for the management of this problem. The Emergency Department physician should read and study both these papers.
Blunt Trauma
ACEP Clinical Policy (Annals 2004, 43:2)
CT
When CT, DPL, and UTS were compared: CT sensitivity 97% and specificity 95%, diagnostic peritoneal lavage sensitivity 100% and specificity 84%, ultrasonography sensitivity 92% and specificity 95%
One Study Shows for small bowel injury, CT scan had a sensitivity of 92% and a specificity of 94% (Am J Surg 1994;168:670-675) Other studies have shown lower sensitivities
CT is not good for detecting blunt pancreatic injury or diaphragmatic injury
(B) CT scan is can not exclude bowel, pancreatic, or diaphragmatic injury
(B) Oral Contrast is not necessary for the CT scan. It may be useful on follow-up scans to evaluate suspected bowel injury
even new gen scanners miss ~20% of intestinal/mesenteric injuries (J Trauma 2008;65:354)
DPL
Has Sensitivity approaching 98-99%. Specificity for blood is ~95%, but specificity for injury requiring intervention is much lower. Can detect as little as 20cc of blood.
(B) Diagnostic peritoneal lavage can be used to exclude hemoperitoneum in blunt abdominal trauma patients. Diagnostic peritoneal lavage does not define the extent of injury, has a 1% to 2% complication rate, and may lead to nontherapeutic laparotomies
Flank bruise=turners, Umbilical bruise=Cullens
DPL-only open with pelvic fx, pregnant, obese, prior surgery
Blunt >100,000 RBC, 20-100=indeterminate
Penetrating >5000 RBC, 1000-5000=indeterminate if risk of diaphragmatic injury otherwise same 100,000. Gunshots=5000.
Should be open or semi-open in pelvic fxs. Should take 5 minutes.
FAST Exam
Novel positioning may increase the sensitivity of the FAST exam. One prospective observational study used increasing aliquots of lavage fluid in hemodynamically stable patients undergoing DPL. Trendelenburg positioning allowed recognition of only 400 cc of intraperitoneal fluid, compared to 700 cc in the supine position.( Am J Emerg Med 1999;17(2):117-120)
Seat Belt Sign
A low-lying transverse abdominal ecchymosis has a strong association with hollow viscus injury and mesenteric tears. In turn, hollow viscus injury often does not produce any pain or tenderness until 6-8 hours following the traumatic event. At a bare minimum, patients with lap-belt contusions should undergo serial abdominal examinations over this time course. Findings of abdominal tenderness should prompt diagnostic study (e.g., abdominal CT and/or DPL) or laparotomy. These perforations often seal up and may not represent for up to 6 weeks in the pediatric population when they come back with bowel obstruction or perforation.
Chance fracture
If you see this lumbar fracture think abdominal injury as well. About 1/3 of patients will have bowel or pancreatic injuries
Who needs a CT
physical exam was not sufficient
J Trauma 2004;57:1072
L Costal Margin Injuries
Injuries to this area have a small but significant risk of intra-abdominal injury (Annals EM 2005;46(3):232)
Abdominal CTs
Allen TL, Cummins BF, Bonk RT, Harker CP, Handrahan DL, Stevens MH. Related Articles, Links Computed tomography without oral contrast solution for blunt diaphragmatic injuries in abdominal trauma. Am J Emerg Med. 2005 May;23(3):253-8. Stuhlfaut JW, Soto JA, Lucey BC, Ulrich A, Rathlev NK, Burke PA, Hirsch EF. Related Articles, Links Blunt abdominal trauma: performance of CT without oral contrast material. Radiology. 2004 Dec;233(3):689-94. Epub 2004 Oct 29. Sharma OP, Oswanski MF, Singer D, Kenney B. Related Articles, Links The role of computed tomography in diagnosis of blunt intestinal and mesenteric trauma (BIMT). J Emerg Med. 2004 Jul;27(1):55-67. Computed tomographic scanning without oral contrast solution for blunt bowel and mesenteric injuries in abdominal trauma. J Trauma. 2004 Feb;56(2):314-22.
Who to Spin
(J Trauma 2005;59(5):1057)
Spin if velocity >20 km/hr
If normal exam, Age<75, and no other injuries to head, spine, legs, or chest; you do not need an abdominal CT
Gluteal Stab Wounds
Can cause intraabdominal injury or vascular damage. May need Abd Ct and Angiogram
Bowel Injury
CT + without oral had >95% sens and spec in prospective trial for bowel injury or mesenteric injury after blunt trauma (J Trauma Volume 56(2) February 2004 pp 314-322)
Pancreas
Ilahi O, Bochicchio GV, Scalea TM, Efficacy of computed tomography in the diagnosis of pancreatic injury in adult blunt trauma patients: a single-institutional study. Am Surgeon 2002;68:7048. We have all been (hopefully) taught that neither a normal appearing pancreas on CT, nor a normal serum amylase, rules out significant pancreatic injury. This paper reports a retrospective review of all blunt pancreatic injuries seen at the Maryland Shock Trauma Center over 5 years. Forty patients with discharge diagnoses of pancreatic injury were found, 19 of whom had had a preoperative CT. All scans were done with both oral and IV contrast on a helical scanner. The CT was positive for pancreatic injury in only 68% (albeit all positive CTs were correct, for a positive predictive value of 100%). The radiologic grade of injury correlated with the actual operative findings also in only 68%, and in the remaining 31% the CT underestimated the injury. Here is more proof that CT is only moderately sensitive for, and does regularly miss or underestimate, pancreatic injury. On the bright side, if the CT is positive, you can take that information to the bank- or better, to the OR.
Free Fluid
In females had a high association with injury (Ultrasound Obstet Gynecol 2005;26:2710
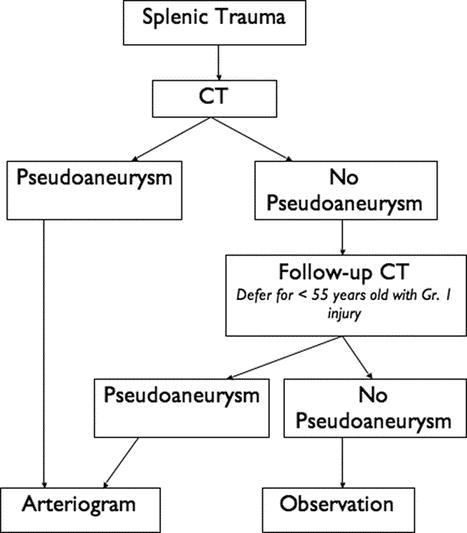
Spleen
Delayed Rupture of Spleen
J Trauma 36(4):568, April 1994.
Am Surg 63:885, Oct 1997
Splenic management fails due to age>55, major grade (3-5), ISS and quantity of hemoperitineum (Multicenter J Trauma 2000 47;1169)
Meguid AA, Bair HA, Howells GA, et al:, Prospective evaluation of criteria for the nonoperative management of blunt splenic trauma. Am Surgeon 2003;69:238-43. Nonoperative management of blunt splenic injury in hemodynamically stable patients is current standard of care. Two reports from 2000 cautioned that the mortality of such management might be increasing, perhaps due to improper triage. The trauma group at William Beaumont in Michigan reviewed in this paper their most current data from prospectively applied criteria for nonoperative management of blunt splenic injury. These criteria which are indeed those used at most centers are (1) hemodynamic stability on admission after initial resuscitation with up to 2 liters of crystalloid infusion, (2) no physical findings or any associated injuries necessitating laparotomy, and (3) a transfusion requirement attributable to the splenic injury of 2 units or less. Ninetynine patients were treated over six years. Thirty-one underwent splenectomy because of hemodynamic instability. Eight of the 68 patients (12%) who were managed nonoperatively developed hemodynamic instability and underwent splenectomy; all failed nonoperative management in the first 72 hours. No patients died from the splenic injury, and there was no associated morbidity from delayed splenectomy. No significant differences in age, sex, mechanism of injury, ISS, blood pressure or hematocrit on admission, transfusion requirements were found between those successfully managed nonoperatively and those who failed. Those failing had a higher mean CT grade of splenic injury, but 29 of 35 patients with a CT grade of 3 or higher were successfully managed nonoperatively. I think this study strongly supports the current criteria stated above.
Haan J, Ilahi ON, Kramer M, et al: Protocol-Driven Nonoperative Management in Patients with Blunt Splenic Trauma and Minimal Associated Injury Decreases Length of Stay. J Trauma 2003;55:317-322 This is a retrospective study of a screening angiography protocol for all patients with CT evidence of blunt splenic injury. All blunt abdominal trauma patients admitted to the R. Adams Cowley Shock Trauma Center over a 3 year period underwent admission abdominal CT, followed by celiac angiography for all those patients with CT splenic injury grade of 3 or more. When a vascular injury was identified, splenic embolization was performed. Angiography performed selectively for higher grade splenic injuries led to a decreased length of stay, higher therapeutic yield, and decreased use of hospital resources without any increase in the failure rate of nonoperative management. In order to fulfill this protocol, serious commitment on the part of the hospital, surgical staff, and vascular radiology staff are absolutely required.
Alejandro KV, Acosta JA, Rodriguez PA, Bleeding manifestations after early use of low-molecular-weight heparins in blunt splenic injuries. Am Surgeon 2003;69:1006-9. Non-operative management of hemodynamically stable patients with blunt splenic injury is the current standard of care. Aggressive prophylaxis against DVT and PE in multiply-injured patients is also the current standard of care. When can low-molecular-weight heparin (LMWH), which is the current prophylaxis of choice, be started when the patient has a splenic fracture? This paper is a retrospective study of all patients with blunt splenic injury managed non-operatively at one institution over 2 years, comparing the outcomes of the 50 patients who received early (during the first 48 hours) LMWH to the 64 who did not. The LMWHs used were enoxaparin 30 mg SQ q.12 hrs. or dalteparin 2500 U SQ qd. The authors found no statistically significant differences in age, gender, ISS, hemodynamic parameters, initial hematocrit, or CT grade of splenic injury between the two groups. They also found that there were no differences in failure of non-operative management (2 of 50 in the early LMWH group vs. 4 of 64 in the no/late LMWH group), number of patients requiring transfusion and mean number of blood units given, morbidity, or mortality. This retrospective study could certainly be flawed by possible selection bias by the attending surgeon as to when to give the LMWH. However, it does strongly suggest that prophylaxis against DVT using LMWH is indeed safe despite the presence of a splenic injury.
abandon non-op management in kids if >20 cc/kg of blood transfusion
observational trial of lmwh in on-op splenic injuries, no increased transfusions or ops (Am surg 2003;69:1006)
vaccinate non-op spleens as it will work better than if you have to give it afterwards. Only really need pneumovax, not all three.
AAST Spleen Injury Score (1994 Revision)
Grade Type Injury Description I Hematoma Subcapsular, <10% surface area Laceration Capsular tear, <1cm parenchymal depth II Hematoma Subcapsular, 10%-50% surface area; intraparenchymal, <5 cm in diameter Laceration Capsular tear, 1-3cm parenchymal depth that does not involve a trabecular vessel III Hematoma Subcapsular, >50% surface area or expanding; ruptured subcapsular or parencymal hematoma; intraparenchymal hematoma > 5 cm or expanding Laceration >3 cm parenchymal depth or involving trabecular vessels IV Laceration Laceration involving segmental or hilar vessels producing major devascularization (>25% of spleen) V Laceration Completely shattered spleen VascularHilar vascular injury which devascularizes spleen
Advance one grade for multiple injuries, up to grade III
(Moore EE et al. J Trauma 1995;38:323.)
Use a sheet of vicryl mesh–cut a keyhole shaped slit from one of its sides, wrapping this around back of the freed up spleen or kidney (meaning it is essential that you first free up the organ of the short gastrics and surrounding Gerota’s so it is only up on its vascular pedicle) so that the keyhole slit comes around the pedicle from the back–sew together the slit then so the keyole encompasses the pedicle, suturing so it is tight, then just keep sewing the free corners and edges together so you have a tight wrap, progressively pulling it tighter and tighter to stop any bleeding.–vicryl works well for this because it is stiff and will really tighten up. The tighter the better–once again, no such thing as an organ compartment syndrome. If there is I must be extraordinarily lucky never to have encountered it in 15 years worth of reapired spleens. You cannot choke off the blood supply–take it is true from 15 years of doing this. ERF
Angio/Embolize grade III and above
Liver
Behaves much differently than spleen, perhaps due to predominantly venous bleeding
recurrent bleeding is usually at 48 hrs
Hemobilia
gi bleeding days to weeks after injury. presents with RUQ pain and jaundice. Get an angio.
Arterial-Portal Vein Fistula
also gi bleed, also angio
Bilioma
try perc drainage
Biliary duct disruptions with associated bileomas, bile peritonitis, biliary leaks, and biliary fistulae are the next most common complication of NOMLI. Pachter and Christmas report a biliary complication rate of 2.8 and 3.2%, respectively.48 and 13 While rarely life threatening, these conditions contribute significantly to the morbidity associated with NOMLI. Bile duct leaks are rarely seen in grades I, II, or III injuries, but are fairly common in grades IV and V. The majority of patients with bile leaks will develop clinical symptoms such as organ failure or worsening abdominal pain. Elevated serum bilirubin during the first week after injury is a harbinger of biliary leak, and will frequently require adjunctive or operative treatment. Wahl et al. has shown that HIDA scanning is nearly 100% sensitive and specific for diagnosing bile duct leaks after NOMLI, especially in patients undergoing AE. They recommend the routine use of HIDA scanning for liver injuries ≥grade IV by postinjury day #4 as a means to early diagnosis and treatment of bile duct injuries. They argue that early diagnosis leads to early intervention, which leads to less invasive adjunctive procedures and ultimately decreased hospital length of stay.69 Percutaneous CT guided drainage has been shown to cure biliary complications about 70% of the time.27 For those who require further intervention, Carrillo et al. advocate non-operative adjuncts in dealing with these leaks, such as endoscopic retrograde cholangiopancreatograpy (ERCP) with stenting, and laparoscopy to relieve biliary peritonitis.10 Goldman recommended operative intervention for biliary complications.28 Regardless of the approach, the underlying principle is adequate drainage of the biliary system. Even a small leak can fill the abdomen over time if the drains are removed prematurely, so it is important to leave them in until the output is essentially zero.
AAST Liver Injury Score
Injury Grade Injury Type/Description I Hematoma: subcapsular, < 10% surface area. Laceration: capsular tear, < 1 cm parenchymal depth. II Hematoma: subcapsular, 10 – 50% surface area, intraparenchymal < 10 cm in diameter. Laceration: capsular tear, 1 – 3cm parenchymal depth, < 10 cm in length. III Hematoma: subcapsular, > 50% surface area, intraparenchymal hematoma > 10cm or expanding .Laceration: 3 cm parenchymal depth IV Laceration: parenchymal disruption involving 25 – 75% of hepatic lobe or 1 – 3 Couinaud segments. V Laceration: parenchymal disruption involving >75% of hepatic lobe or > 3 Couinaud segments within a single lobe. Vascular: juxtahepatic venous injuries (major hepatic veins, retrohepatic vena cava.) VI Vascular:hepatic avulsion.
Advance one grade for multiple injuries
Moore EE J Trauma 1995;38:333.
Embolize grade IV and above
Fabian study would indicate repeat scanning not necessary unless there are signs of complications (J Trauma 2005;59(5):1175)
Intestinal Injury
Wahl found that CT has 100% sensitivity, but included free fluid without source as one of the components (J Trauma 2000 49;380)
Ng had 28 patients with only free fluid without source, 76% therapeutic lap rate (Poster at AAST Oct 2000)
Colon: can repair primarily; no significant difference, but trend towards better outcomes (J Trauma 2000 49;378)
Prospective study of protocol to eval for bowel/mesenteric injuries (Amer J Emerg Med 2006;24:19-24)
If pt has normal mental status–
Perform UTS, if negative: repeat in four hours.
Get CT in
- seatbelt sign
- abnormal UTS
- high velocity/High-risk mechanism
- equivocal abdominal exam
- ongoing blood loss
- hematuria
- prolonged operation for other injuries
(ACS Guidelines)
Signs of BBMI were pneumoperitoneum, unexplained free intraperitoneal fluid, bowel wall thickening, mesenteric fat streaking, and mesenteric hematoma.
If >2 were present, pt was lapped.
If 1 or 2 were present, patient got a DPL:
1 liter infused
Ten minutes later, with at least 700cc back, fluid sent for wbc and rbc
WBC?RBC ratio in the fluid was compared to peripheral blood. A ratio of higher than one was considered positive.
food fibers or bacteria in the fluid was also considered positive (how did they identify bacteria?)
Malhotra showed the free fluid was the most sensitive but not very specific sign of BBMI (J Trauma 2000;48:991)
4From costal margins to inguinal ligaments between anterior axillary lines.
Flank = From 6th intercostal space to iliac crest between anterior and/or posterior axillary lines; Back = From 7th intercostal space to iliac crest posterior to posterior axillary line.
Pancreas
Need to put in post anastamotic feeding tube, so can start feeding soon after surgery.
Give octreotide
Treat the pancreas like a crawfish: suck the head, eat the tail (fabian)
you can just tie off the pancreatic duct of the distal remnant with little problem-
Gentilello LM, Cortes V, Buechter KJ, Gomez GA, Castro M, Zeppa R. Whipple procedure for trauma: is duct ligation a safe alternative to pancreaticojejunostomy? J Trauma. 1991 May;31(5):661-7; discussion 667-8. Review.
Alternatively there is work form the Durban Unit in South Africa which suggests inplanting the pancreas body/tail into the posterior stomach. See Injury. 2000 Jun;31(5):394-5.
IVC
ivc walk up with intestinal allis clamps (J Trauma Henry S 2001)
Penetrating Trauma
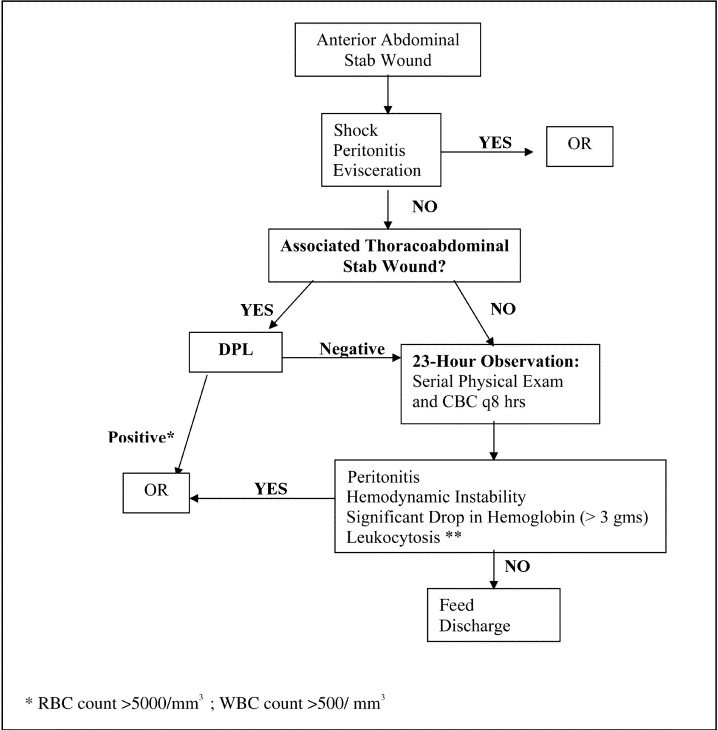
Observation
The patient is admitted for observation for 24 hours. During this time the patient is has frequent (hourly), regluar checks of their haemodynamic status. The abdomen is examined routinely for signs of developing peritonitis. Ideally the same surgeon should examine the patient each time. If this is not possible, during a handover period both surgeons should examine the patient at the same time so they agree on the current status of the abdomen and whether there has been any progression in symptoms. The timing of examinations varies inthe literature, but should probably start out more frequently and then decrease over time. A suggested sequence of examination might be at 1, 4, 12 and 24 hours after the initial assessment. Some authors recommend examination every four hours. (trauma.org)
Retrsopective study would indicate 12 hour observation time (J Trauma 2005;58(3) March 2005 pp 523-525)
Local Wound Exploration
Local wound exploration (LWE) requires a formal evaluation of a stab wound under local anaesthesia. This procedure is usually performed in the operating room, but is performed in the emergency department by some institutions. The wound is extended under local anaesthesia and the track followed through tissue layers. Penetration of the anterior fascia is considered a positive LWE, as penetration of the peritoneum is difficult to identify. A positive LWE leads to either laparotomy or another diagnostic test such as DPL or laparoscopy. When LWE is used alone to determine laparotomy, there will be a high non-therapeutic laparotomy rate. Even if the peritoneam is penetrated were used as a cut-off, many of these patients will have no intra-peritoneal injury, or an injury that does not require surgical intervention – most commonly omental laceration, mesenteric laceration or liver tears that have stopped bleeding. DPL
between 5000/ml and 20,000/ml
FAST CT Scan
Kenji just published an article on observation vs. CT; obs was better: Prospective Evaluation of the Role of Computed Tomography in the Assessment of Abdominal Stab Wounds (JAMA Surg. 2013;():-. doi:10.1001/jamasurg.2013.2521.)
Flank or back wound
Flank or back wounds may be associated with injuries to retroperitoneal organs such as the colon, kidney and lumbar vessels as well as ureters and the major vascular structures
– or more rarely the pancreas, aorta and inferior vena cava. Of these, the colon is the injury most often missed. Where colon injury is a possibility, the duration of serial physical examination is extended to 72 hours, watching for fever or a rise in the white cell count. An alternative is to perform a triple-contrast CT scan. Where the wound track extends up to the colon, or there is evidence of abnormal bowel wall thickening, laparotomy is indicated.
Update on flank wounds (Am Surg 2005;71:493)
study of triple ct for back and flank showed no missed operative wounds (Injury Volume 40, Issue 1, January 2009, Pages 48-53)
Wound to buttock or perineum
The most dangerous missed injury here is the occult rectal injury. Any penetrating injury to the gluteal region carries the risk of rectal injury. Digital rectal examination is inadequate and full proctoscopy and sigmoidoscopy should be performed, looking for the presence of blood and/or a mucosal tear.
Non-operative management of gunshot wounds (Ann Emerg Med 43(3):344, March 2004)
CT Tractogram
for tangential abd gsws (J Trauma 2006;60(6):1362)
apply metal wound markers
10 F foley into entrance wound
gently inflate balloon
150 cc water-soluble contrast into tract
clamp foley
ct with triple contrast
after done, flush tract with saline
Operative Management
Prep chin to knees to the post ax line
Three cuts to open from xiphoid to pubis. Just superior to umbilicus is peritoneal defect, can push through with a finger
eviscerate the bowel, then pack the four quadrants
the supraceliac aorta can be compressed through a hole in the lesser omentum
supramesocolic=liver/stomach/spleen
inframesocolic=small bowel/colon/bladder
kocher maneuver mobilize the duodenal loop and head of the pancreas, take down lig of treitz, put hole in L side of omentum
mattox maneuver l sided medial visceral rotation
cattell brasch=super extended kocher
pringell-poke hole in lesser omentum to l of triad, pinch triad, you can clamp with vascular clamp, you have~30 min
abd stab wounds
1/3 penetrate
1/3 penetrate and cause intraperitoneal injuries
1/3 don’t
if it does penetrate, can perform serial exams=serial crits, hourly vital signs, and q 4 hour exams for 24 hours
consider marking the tender area to clarify any changes
or do dpl
cutoff is 1000-10,000 cells/dl
non-op gsw
can consider for r thoracoabdominal injuries as they usually hit only lung, liver, and a protected diaphragm
also low pelvis if trajectory can be determined to be extraperitoneal and sigmoidoscopy, cystography, and ct are negative
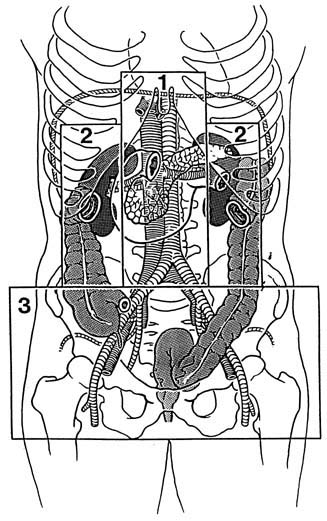
Retroperitoneal Hemorrhage
Retroperitoneal Hemorrhage Tutorials — Educational Resources There are 3 retroperitoneal zones. Zone 1: the midline retroperitoneum Zone 2: the perinephric space Zone 3: the pelvic retroperitoneum Zone I A hematoma in zone 1 mandates exploration because of the high likelihood of major vascular injury in this area. The transverse mesocolon divides supra from inframesocolic zone 2 hematomas. A supramesocolic hematoma is the result of injury to the suprarenal aorta, celiac axis, proximal SMA, or proximal renal artery. A inframesocolic hematoma is the result of injury to the infrarenal aorta or IVC. Vascular control supramesocolic: clamp or compress the aorta at the diaphragmatic hiatus, exposure of injured vessels by a left sided medial visceral rotation inframesocolic: clamp or compress supraceliac aorta and provide exposure by opening the midline posterior peritoneum Zone II A hematoma in zone 2 is usually the result of injury the the renal vessles or parencyhma and mandates exploration if from penetrating injury. A non-expanding stable hematoma resulting from blunt trauma is better left unexplored. Indications for exploration of zone II retroperitoneal hematoma are: 1. expanding or pulsatile hematoma 2. urinary extravasation 3. unstable patient 4. penetrating injury Vascular control requires midline looping of the ipsilateral artery and vein between the aorta and IVC. This is time consuming however, so in presence of active hemorrhage, mobilize kidney by incising the posterior peritoneum and Gerota’s fascia lateral to it and then elevate the kidney medically and clamp the entire renal hilum. Zone III A hematoma in zone 3 from penetrating injury mandates exploration because of likely iliac vessel damage. Blunt trauma injuries should not usually be explored because they are associated with pelvic fracture.

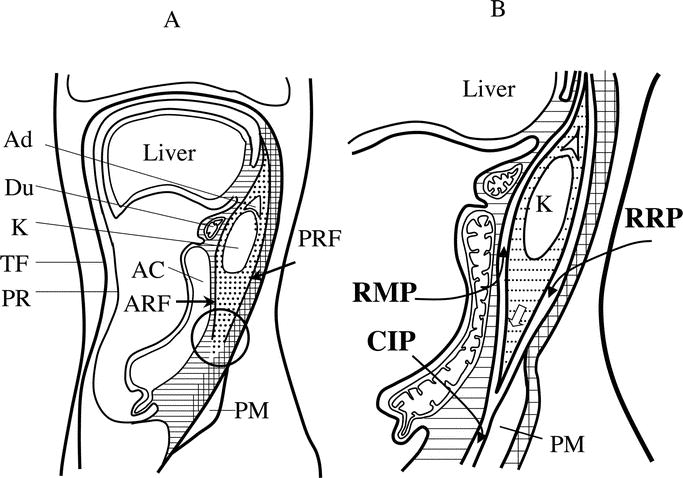
Cross-sectional diagrams of the retroperitoneal space. Diagrams at the level of the left renal hilus illustrate cross-sectional anatomy of the medial and left parts of the retroperitoneum. (A) Traditional tricompartmental theory.15 Anterior pararenal space (APS) (striped area), perirenal space (PRS) (stippled area), posterior pararenal space (PPS) (cross-hatched area), anterior renal fascia (ARF), posterior renal fascia (PRF), and lateroconal fascia (LCF). P, pancreas; IVC, inferior vena cava; PR, peritoneum; DC, descending colon; K, kidney; Ao, aorta; TF, transversalis fascia. (B) New concept of interfascial planes.11,12 This diagram depicts interfascial planes as curved arrows among the APS, PRS, and PPS: the retromesenteric plane (RMP), corresponding to the ARF; the retrorenal plane (RRP), corresponding to the PRF; and the lateroconal plane (LCP), corresponding to the LCF. The RMP spreads beyond the midline, providing a route for contralateral spread of RH (bidirectional arrow). The RMP, RRP, and LCP communicate at the fascial trifurcation (FT). Note that the PRS is closed medially (open arrow). Figure reprinted with permission from the American Roentgen Ray Society11,12 and Springer Science and Business Media15. From: Ishikawa: J Trauma, Volume 59(3).September 2005.595-608
Rectal Trauma
Blunt anorectal trauma is exceedingly rare; these are results of penetrating trauma
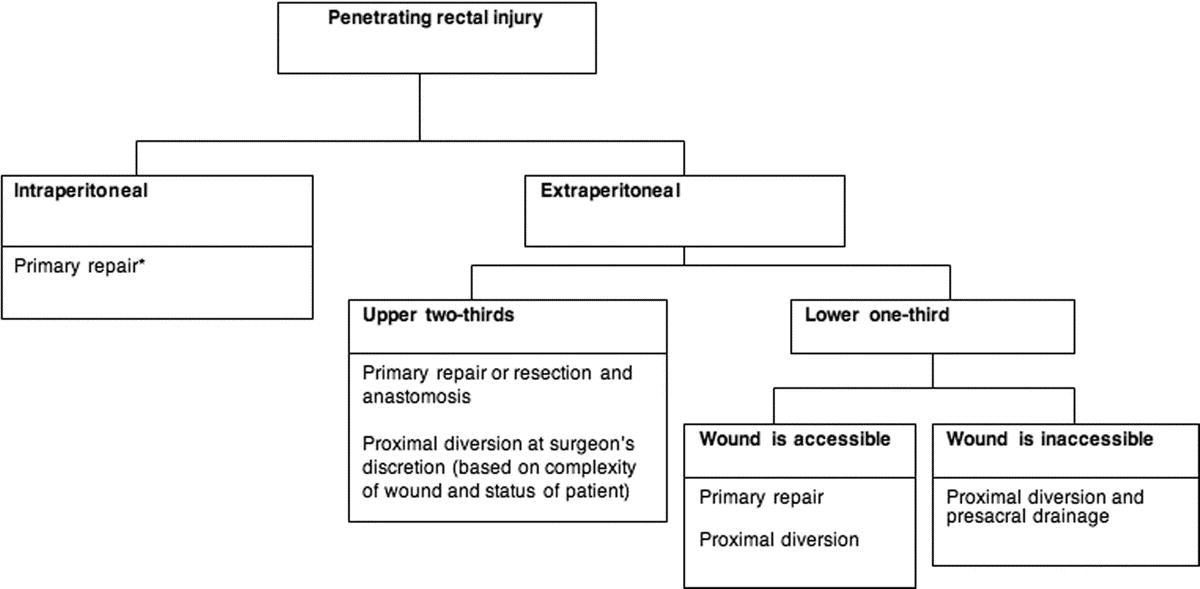
Intraperitoneal Rectal Injuries
treat like any colonic injury
Most can be primarily repaired without diversion
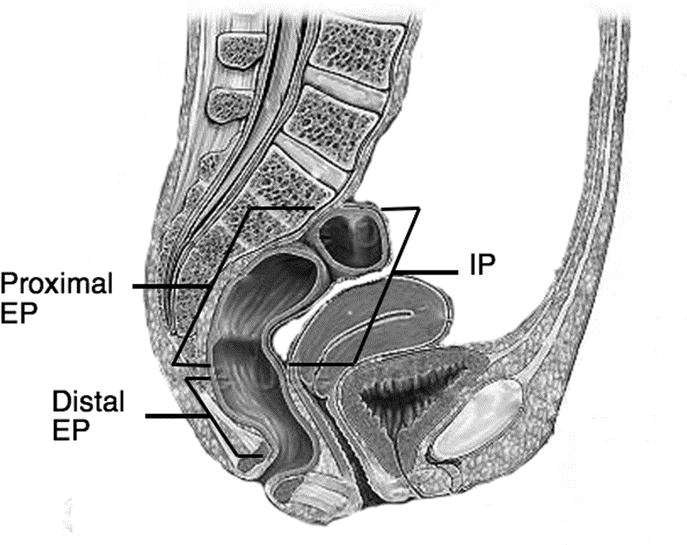
Extraperitoneal Rectal Injuries
Upper 2/3 can usually be repaired with plus/minus diversion
For lower 1/3
classic management diverting sigmoidostomy, presacral drainage, and rectal washout
loop ostomy is sufficient for this purpose
if explored, presacral drainage is not necessary
if not explored, presacral drainage is required to prevent retrorectal abscess formation
(J Trauma 2006;60:508)
Anal Canal
unless extensive, they do not need an ostomy
retrospective study shows time to lap increases mortality especially in the 60-90 minute range
Fascial Ultrasound for anterior abdominal stab wounds (J Trauma2005;59(4):843)


Ligate the portal vein and the entire bowel turns massively edematous
Richardson JD. Changes in the management of injuries to the liver and
spleen. J Am Coll Surg 2005;200:648-669.
This was the annual Scudder Oration on Trauma given at the 2005
Congress of the American College of Surgeons. Dr Richardson, one of the
real deans of trauma care, reviewed the changes in the management of injuries
of the liver and spleen that have occurred in the past half-century. We no
longer rely upon physical examination to detect intra-abdominal blood; that
function has been replaced by US, which is much more accurate. Even better
and foremost among all the changes because it is the basis upon which all
nonoperative management rests, is the use of CT. Nonoperative management
of both liver and spleen injuries is now the accepted, even ”politically
correct,” default position. The only real indications for operation are
The Literature of Emergency Medicine 533
hemodynamic instability and/or concomitant hollow viscus injury. Angiography
is now widely used for control of hemorrhage, and laparoscopic and
US- or CT-guided drainage of collections have proven quite useful.
Nonoperative management of liver injuries has been especially successful.
Nonoperative management of splenic injuries is more controversial and
remains not as well proven in Dr Richardson’s view. First of all, it is unclear
what the real incidence of overwhelming postsplenectomy infection in the
adult is. Moreover, there is a real difference in what happens to injured
spleens during the first week after injury, as compared with the injured liver;
true delayed bleeding and even free rupture is a real concern for injured
spleens, much more so than for injured livers. Nonoperative management of
the ruptured spleen should be appropriately used but not at the risk of
threatening the patient’s life. This excellent article, which reviews what has
happened in the last 40 years, is both educational and enjoyable to read.
Christmas AB, Wilson AK, Manning B, et al. Selective management of blunt
hepatic injuries including nonoperative management is a safe and effective
strategy. Surgery 2005;138:606-611.
Five hundred sixty-one patients with blunt hepatic injuries seen over the
10-year period (1993 through 2003) were reviewed in this article from the
trauma group at the University of Louisville (Louisville, Ky). Fifty-nine
percent had grade 1 or 2 injuries. Most of these were managed
nonoperatively; the ones who were operated on went to surgery for other
abdominal injuries, and there were no liver-related deaths. Two thirds of
patients with grade 3 or 4 liver injuries and one third of patients with grade
5 injuries were managed nonoperatively, with a mortality of only 2.2%.
Patients who required operation because of hemodynamic instability or
concomitant injuries had a mortality of 30%. Eleven percent of the 378
patients managed nonoperatively required adjunctive procedures. Twelve
patients underwent angioembolization for bleeding, all within the first
24 hours after injury. All of these patients had grade 3 injuries or higher,
and 11 of the 12 survived. Laparoscopic or percutaneous drainage of
bilomas or blood collections was performed in 18 patients. Endoscopic
retrograde cholangiopancreatography (ERCP) was needed in 12 patients,
8 of whom required a stent, and 1 required operative repair of a completely
transected left hepatic duct.
Among the important points emphasized in this article are the following:
1. Hemodynamic stability is a sine qua non for nonoperative management;
it is actually a sine qua non for even getting a CTscan which, of
course, is the basis for any nonoperative management. The authors of
this study defined as hemodynamically stable those patients who
maintained, or regained after 2 L of IV crystalloid, a systolic BP
greater than 90 mm Hg and a heart rate less than 100.
2. Patients who lose hemodynamic stability need to be taken to
angiography for embolization, if it is known from the CT that liver
bleeding is the source of the problem, or to the OR if th
Alzamel HA, Cohn SM. When is it safe to discharge asymptomatic patients
with abdominal stab wounds? J Trauma 2005;58:523-525.
If we decide to observe patients with abdominal stab wounds, how
long do we have to observe them? The authors of this article reviewed a
prospectively collected trauma registry database and reviewed the
medical records of 650 hemodynamically stable patients who presented
over a 7-year period. Sixty-eight patients (11%) required surgical
intervention. One third underwent surgery within the second hour of
presentation, one third had surgical intervention between the second and
fourth hours, and only 13% had abdominal intervention between the
fourth and sixth hours. Only 1 patient showed signs of hemodynamic
instability from hemoperitoneum from a stab wound 12 hours after
admission, and no patients required abdominal surgery after 12 hours of
close observation. The authors conclude that after 12 hours of close
monitoring and serial physical examinations, if no signs of hemoperitoneum
and instability arise, the patient can be discharged from the
hospital. I disagree to this conclusion, having personally cared for several
patients, and having read about many more, with hollow viscus injuries
whose peritonitis and signs of inflammation/infection did not appear for
more than 24 hours. If you discharge people before this time, you better
be sure they are reliable and will return to your ED immediately if they
develop worsening symptoms.
Dissanaike S, Griswold JA, Frezza EE. Treatment of isolated penetrating
flank trauma. Am Surg 2005;71:493-496.
The authors of this article were interested in formulating a new
algorithm for evaluation of patients with stab wounds of the flank. They
reviewed the records of the 23 patients they had seen over the previous
5 years and found that triple-contrast CT scan was the preferred method,
except in those patients in whom the stab wound was above the bottommost
rib, in which case, laparoscopy was required to rule out diaphragmatic
injury. This is actually correct, but not news. The proper definition of
flank
is the area between the 12th rib and the iliac crest and between the anterior
and posterior axillary lines. The authors’ definition was between the fifth
intercostal space and the iliac crest; I would call injuries above the
lowermost rib here thoracoabdominal stab wounds, not flank wounds, for
the same reason the authors advocate laparoscopy: the diaphragm is at risk
in the area above the 12th rib. So, whatever one’s definitions are, if the stab
wound is in the ribs, one must evaluate the diaphragm. If the stab wound is
below the ribs, and posterior to the anterior axillary line, then triple-contrast
CT is the way to go.
e source is
unknown or if there is a suspicion of other intra-abdominal injuries.
Whole body imaging in blunt multisystem trauma patients without obvious signs of injury Arch Surg 2006;141:46875
This prospective observational study from Los Angeles County and the University of Southern California Medical Center was conducted from January 2004 through June 2005. The purpose was to investigate the utility of whole-body computed tomography (CT) imaging in patients who were hemodynamically stable and had no obvious signs of chest or abdominal injury but suffered high mechanisms of injury. Each patient underwent a CT of the head, cervical spine, and chest, abdomen, and pelvis. One thousand patients were included during this time period. The inclusion criteria were: 1) no visible evidence of chest or abdominal injury; 2) hemodynamic stability; 3) normal abdominal examination results in neurologically intact patients or unevaluable abdominal examination results secondary to a depressed level of consciousness; and 4) significant mechanism of injury. The latter criteria is defined as: 1) motor vehicle collision at greater than 35 mph, 2) falls greater than 15 feet, 3) automobile hitting pedestrian with pedestrian thrown more than 10 feet, and 4) assaulted with a depressed level of consciousness. Of the 1000 patients enrolled, 592 were enrolled based on mechanism of injury. In other words, these patients were evaluable and had a normal level of consciousness. CT of the head was abnormal in 3.5% of the patients. CT of the cervical spine was abnormal in 5.1%. CT of the chest was abnormal in 19.6%. CT of the abdomen and pelvis was abnormal in 7.1%. Furthermore, the authors report that the overall treatment was changed in 18.9% of the patients. Such changes include early discharge from the Emergency Department, release to other services, admission for serial examinations, performance of additional diagnostic studies or interventions, and immediate operative intervention. Despite the cost and radiation exposure associated with CT scanning, the authors conclude that the use of the pan scan based on mechanism of injury is justified in the awake and evaluable patient. Comment: Despite the advancement of medical imaging, injuries may still be missed by CT scanning. It is important to include every aspect of the patients evaluation in the final decision-making process, and not rely solely on the results of the imaging studies.
Non-operative Management of Penetrating Abd Trauma
(Ann Surg 2006;244:620)
prospective case series
gsw and stabs
ct findings of need for lap: free air, free fluid in absence of solid organ injury (????), localized bowel thickening, bullet tract close to hollow viscus with surrounding hematoma, contrast blush with hemodynamic instability

clinically unevaluable pts should not be consider for non-op
Abdominal Stab Wounds
Anterior
Local wound exploration followed by either
A) discharge home if the wound didn’t penetrate or
B) admission for observation/serial examination if it did,
*actually works*, and works well *as long as one is willing to put in the time and effort to re-examine the patient* (every four hours is what I do for the first twelve hours or so, then every six hours until 18-24 hours have passed) and one strictly adheres to clear-cut indications for exploration, such as progressive abdominal tenderness, fever, increasing leukocytosis, vomiting, distention, etc. I just can’t accept the argument that mandatory laparotomy for all patients with peritoneal violation (be it shown via local wound exploration or by laparoscopy) is the best thing for the patient. It might be the best thing for the surgical resident needing to learn technique, or the attending surgeon wanting to quickly ‘know’ one way or the other if an injury is there so that he/she can go home and stop worrying. But a negative laparotomy is a morbid procedure that should be avoided if it can safely be avoided. As for ometal evisceration, I prefer to explore them all, if for no other reason than to properly close the fascial defect, which is usually pretty large. I refer you to a good paper by
Kimberly Nagy (*Nagy K, Roberts R, Joseph K, An G, Barrett J. Evisceration after abdominal stab wounds: is laparotomy required? J Trauma 1999 Oct;47(4):622-4; discussion 624-6d*) as support for my bias in this particular scenario. Finally, let’s not forget that DPL (does anyone remember DPL?) can be used to screen these patients as well. I refer you to the classic article by Feliciano (*Feliciano DV, Bitondo CG, Steed G, et al. 500 open taps or lavages in patients with abdominal stab wounds. Am. J Surgery** 148:772, 1984*) and a more recent one
(*Zantut LF, Ivatury RR, Smith RS, et al. Diagnostic and therapeutic laparoscopy for penetrating abdominal trauma: a multicenter experience. J Trauma**, 1997 May, 42(5) 825-9.*). Laparsocopy is nice, but it’s indications in trauma have been exaggerated. Then again, I could be all wrong about this…. C. Ursic Santa Fe USA —
Horrible article on FAST for strat of pelvic trauma. misses the entire point (J Trauma 2007;63:97)
Peritonitis
Hemodynamically “stable” patients with peritonitis after penetrating abdominal trauma: identifying those who are bleeding.
Brown CV, Velmahos GC, Neville AL, Rhee P, Salim A, Sangthong B, Demetriades D.Department of Surgery, Division of Trauma and Critical Care, University of Southern California Keck School of Medicine, Los Angeles County/University of Southern California Medical Center, 1200 N. State Street, Los Angeles, CA 90033, USA. carlosbr@usc.edu
HYPOTHESIS: Despite initial presentation, hemodynamically stable patients with penetrating abdominal trauma may have significant ongoing hemorrhage and major intra-abdominal injuries requiring emergent surgical intervention. DESIGN: Cohort analytic study. SETTING: Academic, level I trauma center. PATIENTS: One hundred thirty-nine consecutive hemodynamically stable patients with penetrating abdominal trauma in whom peritonitis was the sole indication for laparotomy. MAIN OUTCOME MEASURES: The primary outcome was the amount of blood initially found at laparotomy. Secondary outcomes included additional intraoperative blood loss, intraoperative hypotension, transfusion, fluid, and vasopressor requirement; need for admission to the intensive care unit and mechanical ventilation; complications; survivor length of stay in the hospital and intensive care unit; and mortality. RESULTS: The admission systolic blood pressure (mean +/- SD, 131 +/- 22 mm Hg) and heart rate (mean +/- SD, 91 +/- 22 beats/min) were normal. Median time from peritonitis to incision was 40 minutes. Ninety-seven percent of patients had intra-abdominal injury, including 81%, hollow visceral; 36%, solid organ; and 11%, vascular injury. Though most patients had less than 750 mL(3) of blood found initially at laparotomy, there were 11% with 750 to 1500 mL(3) and 7% with 1500 mL(3) or more. Intraoperative hypotension (25%) and blood transfusion (39%) were common. Postoperatively, 40% of patients required intensive care (78% of them requiring mechanical ventilation) and 19% required additional transfusion within 24 hours. Complications occurred in 25% of patients, with intra-abdominal abscess (12%) and wound infection (7%) being the most common. Three patients died, 2 of exsanguination and 1 of multisystem organ failure. CONCLUSIONS: Following penetrating abdominal trauma, peritonitis should be a trigger for emergent operation regardless of vital signs, because hemodynamic “stability” does not reliably exclude significant hemorrhage. Vascular injury, subsequent hypotension, blood transfusion, and complicated postoperative course are common in this population.
Obs time for flank stabs
Am Surg. 2007 Jan;73(1):25-31.Links
What is the optimal observation time for a penetrating wound to the flank?
MacLeod J, Freiberger D, Lewis F, Feliciano D.
Department of Surgery, Emory University, School of Medicine, Atlanta, Georgia, USA.
Options for a hemodynamically stable patient with a penetrating wound to the flank or back but no peritonitis, includes serial physical examinations versus a triple-contrast CT scan. There is, however, little consensus on the minimum time for serial examinations to exclude an injury that requires an operation. Therefore, a retrospective review of patients who sustained a penetrating wound to the flank or back and were admitted to a Level I trauma center was performed. Patients were identified through the trauma registry, patient charts, and morbidity/mortality records. From 1995 to 2003, 93 patients undergoing observation for a penetrating flank/back wound subsequently required a therapeutic laparotomy. The time from admission to operation was less than 3 hours for 84 per cent of the patients requiring therapeutic intervention. A further 10 per cent presented with symptoms between 4 to 6 hours, and 6 per cent between 7 to 18 hours. All the injuries caused symptoms within 18 hours of the injury event. The majority of patients (94%) who require a laparotomy after a period of observation for a penetrating flank/back wound will develop signs and symptoms within 6 hours of admission. A period of hospitalization longer than 18 hours did not detect further injuries in the asymptomatic patient.
Non-recon ct is good enough for thoracolumbar spine fxThe Journal of Trauma: Injury, Infection, and Critical Care
Issue: Volume 69(1), July 2010, pp 119-121
Abd Injuries without Hemoperitoneum
(J Trauma 1997;42(4):617)
Retroperitoneal Planes
Finally a validation of 6-hours of serial exam in abd stab wounds (JAMA Surg. 2013;148(9):810-816)