“All things are poison and nothing is without poison. Solely the dose determines that a thing is without poison.”
–Paracelsus
Tox Links
www.householdproducts.nlm.nih.gov
www.microdex.com/products/poisondex
www.clinicalpharmacology-ip.com
Mnemonics
Do not adsorb to charcoal
PHAILS
Pesticides;
Hydrocarbons;
Acids and alkali;
Iron;
Lithium; and
Solvents
Repeat Dose Charcoal
ABCD
Antimalarials (quinine) and aminophylline (theophylline);
Barbiturates (Phenobarbital) and beta-blockers (nadolol);
Carbamazepine
Dapsone
and Dilantin (Phenytoin)
Valproate
Theophylline
Toxins Accessible To Hemodialysis
Small Molecule, Low Protein Binding, Water Soluble
I STUMBLE
Isopropyl Alcohol
Salicylates
Theophylline (caffeine)
Uremia
Methanol
Barbiturates, beta-blockers (water soluble, such as atenolol)
Lithium
Ethylene glycol
Vital Sign/PE Mnemonic
s
Bradycardia (PACED)
Propranolol or other beta-blockers, poppies (opiates), propafenone, phenylpropanolamine
Anticholinesterase drugs
Clonidine, calcium-channel blockers
Ethanol or other alcohols
Digoxin
Tachycardia (FAST)
Free base or other forms of cocaine
Anticholinergics, antihistamines, amphetamines
Sympathomimetics (cocaine, amphetamines), solvent abuse
Theophylline
Hypothermia (COOLS)
Carbon monoxide
Opiates
Oral hypoglycemics, insulin
Liquor
Sedative-hypnotics
Hyperthermia (NASA)
Neuroleptic malignant syndrome, nicotine
Antihistamines
Salicylates, sympathomimetics
Anticholinergics, antidepressants
Hypotension (CRASH)
Clonidine, calcium-channel blockers
Reserpine or other antihypertensive agents
Antidepressants, aminophylline
Sedative-hypnotics
Heroin or other opiates
Hypertension (CT SCAN)
Cocaine
Thyroid supplements
Sympathomimetics
Caffeine
Anticholinergics, amphetamines
Nicotine
Rapid respiration (PANT)
PCP, paraquat, pneumonitis (chemical)
ASA and other salicylates
Non-cardiogenic pulmonary edema
Toxin-induced metabolic acidosis
Slow respiration (SLOW)
Sedative-hypnotics (including GHB)
Liquor
Opiates, sedative-hypnotics
Weed (marijuana)
Miosis (COPS)
Cholinergics, clonidine
Opiates, organophosphates
Phenothiazines, pilocarpine
Sedative-hypnotics
Mydriasis (AAAS)
Antihistamines
Antidepressants
Atropine and other anticholinergics
Sympathomimetics
Drugs Causing Pneumonitis Or Pulmonary Edema
(MOPS)
Meprobamate, methadone
Opiates, organophosphates
Phenobarbital, propoxyphene, phenothiazines
Salicylates, smoke inhalation (including cocaine smoke), solvents
Causes of high Osmal Gap
ME DIE
Methanol
Ethylene glycol
Diuretics (osmotic diuretics like mannitol)
Isopropyl alcohol
Ethanol
Also acetone
Drugs that cause Seizures
Aspirin
Tramadol (Ultram®, Ultracet)
Tricyclic antidepressants
Bupropion (Wellbutrin®, Zyban®)
Diphenhydramine (Benadryl®)
Amphetamines/Cocaine
Venlafaxine (Effexor®)
Leon from the Poison Review has this mnemonic:
O – organophosphates
T – tricyclic antidepressants
I – isoniazid, insulin (hypoglycemia)
S – sympathomimetics, synthetic cannabinoids (Spice)
C – cocaine, camphor
A – amphetamines, anticholinergics, atypical antipsychotics
M – methylxanthines (theophylline, caffeine)
P – phencyclidine (PCP)
B – botanicals (e.g., water hemlock), bath salts, benzo withdrawal, bupropion
E – ethanol withdrawal
L – lead, lindane
L – lithium, lidocaine
Smells of Toxicology (River’s)
Nitrites, Isopropyl alcohol: fruit like
Phenols: disinfectant
Cyanide: bitter almonds
Chloral Hydrate: pear-like
Arsine, phosphorous, tellerium, organophosphates: garlic
Turpentine: violets
Hydrogen Sulfide: rotten eggs
Camphor, naphthalene: mothballs
Phosgene: hay
Methylsalicylate: wintergreen
Presentations
Brady+Vomiting=Digoxin
Also av or nodal block with atrial or ventricular irritability
Tachy+Vomiting=think theo
Extrapyramidal Toxidrome
TROD seen with zines, haldol, reglan
Tremor, torticollis, trismus
Rigidity
Opisthotonos, Oculogyric Crisis
Dysphonia, dysphagia
Activated Charcoal
AC only helps in tylenol overdose if given within 1 hour of ingestion (J Toxicol Clin Toxicol 2001;39(6):601)
Position Statement Am Acad Toxicol, no AC after 1 hour can be supported by evidence, only give in patients with intact or protected airway
A different opinion on charcoal
Doesn’t adsorb charged ions (potassium, sodium, etc.)
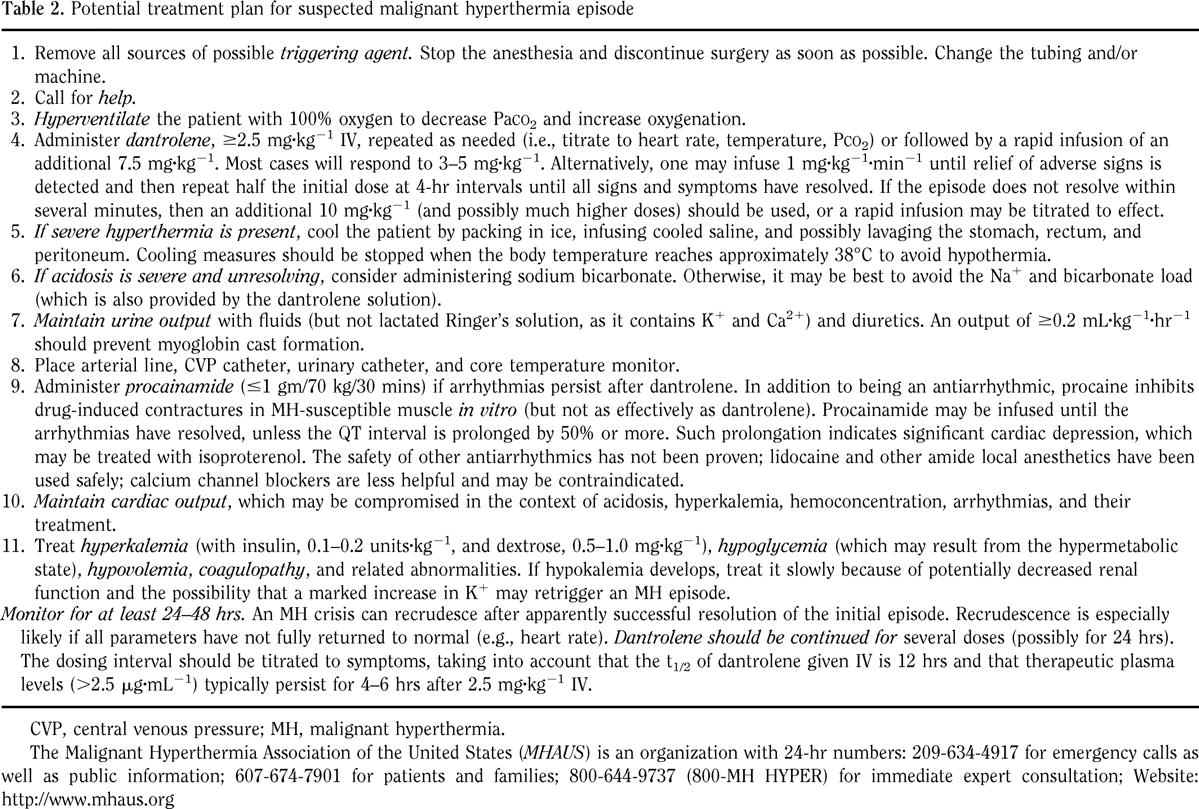
Malignant Hyperthermia
Rare inherited disorder: autosomal dominant with variable expression and incomplete penetrance
May occur up to 24 hours after the use of succinylcholine or inhaled anesthetics
From abnormal calcium channels
AMS, rigidity, hyperthermia, autonomic instability, acidosis
Active Cooling
Benzos
Dantrolene-1 mg/kg IV may repeat to dose of 10 mg/kg. 2 mg/kg PO QID for 2 days after.
Date Rape Drugs
GHB and flunitrazepam
Barbs, benzos, ambien, carisoprodol, chloral hydrate, GHB, THC, Cocaine, methamphetamines, XTC, PCP and Ketamine, Scopolamine
Statins
Cholesterol membrane instability, muscle affected most
Rhabdomyolysis b/c of coenzyme Q inhibition in mitochondria. Myopathy and hepatotoxicity
.
TB Meds
Isoniazid (INH)
>20 mg/kg needs evaluation
>79 mg/kg can lead to seizures
May be asymptomatic for up to 2 hours post ingestion
N/V, photophobia, hallucinations, dizziness, ataxia, slurred speech, lethargy progressing to grand mal seizures, coma, and death
Blocks GABA formation (active b6 catalyzes glutamate to GABA, INH makes you pee out B6 and decreases enzymatic formation of active B6), also inhibits conversion of lactate to pyruvate, so lactic acidosis
Benzos
Pyridoxine (B6) should be administered to match gram for gram dose of INH up to 5 grams. If dose unknown, give 5 grams empirically
Effects diminish rapidly, so 6 hours observation, then D/C
Side effect is hepatitis: 10% have elevated enzymes, 10% of those get hepatitis, 10% of those die from it.
Can also cause niacin deficiency: pellagra=diarrhea, dementia, dermatitis
Rifampin
Causes all fluids to turn red
Ethambutol
Optic Neuritis
Pyrazinamide
Hepatic dysfunction
Antimalarial Meds
Mefloquine
gives vivid dreams
Quinine
Cinchoism=n/v, hearing loss, tinnitus, HA.
Also blocks Na and K channels in heart causing QRS/QT prolongation, requiring Bicarb. TDP as well. Give MdAC. Can get blindness from direct retinal toxicity.
Chloroquine
GI Symptoms, Hypokalemia, QRS/QT prolongation, severe hypotension. Give 2 mg/kg diazepam over 30 min then 1-2 mg/kg/day. EPI .25 ug/kg/min until systolic > 100. Validated in France where this used to be a popular suicide med.
May want to supplement K/Mg before giving bicarb to avoid exacerbating K-channel blockade
Dapsone
MetHb
Paraphenylenediamine (Para, PPD)
In hair dyes
Respiratory failure, myoglobinuria, vomiting, tongue swelling. Causes cancer.
Hydrazine
can cause stat epilepticus, contained in jet fuel
Baclofen
Withdrawal
Fever, AMS, rebound spasticity, rhabdo, organ failure
Can be caused by catheter malfunction, empty reservoir, dead batteries
RX: restart the pump, oral baclofen, benzos
Poisonings in Lab workers
CO, Cyanide, Azides, MetHb inducing chemicals
Fatal inhalations-CO, Hydrogen Sulfide, Asphyxiants, NOs, Smoke, Halogens
Blood Screening-Na Azide, cyanide, CO, sulfide
Sodium Azide (NaN3)
Highly toxic and highly explosive
Used in detonators and as preservative in lab reactions
In vapor form, colorless, pungent.
Sx arise suddenly and dissipate in a few hours
ABD cramps, chest pain, dysphoria, faintness, flushing, headache, incontinence, n/v, palpitations, weakness, agitation, diarrhea, hyperventilation, hypo or hypertension, leukocytosis, pallor, syncope, sweats, tachycardia, and vomiting. Larger doses can give blindness, dilated pupils, NCPE, myocardial dysfunction, myocarditis, shock, seizures and coma. Uncouples oxidative phosphorylation.
GI Decon and supportive care
Mitochondrial Toxins
propofol
b. cereus toxin
valproate
hiv meds
can see ketoacidosis, lactic acidosis, myopathy
Propofol Infusion Syndrome
Inten Care Med 2003;29:1417
cardiac depressant
infusion syndrome is associated with catecholamine and steroid tretament simultaneous with propofol
consider after >48 hours of infusion
catechols-increased CO causes increased clearance requiring higher doses
Causes cardiac failure and rhabdomyolysis
>5 mg/kg/hr is considered high dose and puts pts at risk
Often seen in kiddies, but reported in adults (Burow BK – Anesthesiology – 01-JUL-2004; 101(1): 239-41 followed by editorial comment)
Green Urine is Seen
Phase 1. Fast distribution from blood to tissue; half-life, 2 to 3 minutes
The desired clinical response can be titrated by either bolus injections of 0.5 mg/kg every 10 seconds to a total dose of 2 to 2.5 mg/kg or by continuous infusion.
Although hypotension is the most commonly reported adverse event, volume loading with 12 mg/kg of Ringers lactate solution is effective in maintaining hemodynamic stability.18 Interestingly, propofol in high doses has also been rarely reported to cause seizures, but the mechanism is unknown.19,20
Annals EM Dec 2003 42:6; 793. propofol recovery time is 5-15 minutes with a 30 second onset
strong anti-emetic properties
can cause hypotension, apnea, and pain on injection
Bassett Peds Study-hypoxia in 5%, airway repositioning in 2% and apnea needing BVM in .8%
Great review of lit
Propofol (2,6 di-isopropylphenol) is a very short acting non-opioid sedativehypnotic agent. It is thought to work by potentiating the binding of -amino butyric acid to receptor sites in the central nervous system (CNS).6 It has no analgesic properties and must be used in conjunction with adequate pain relief. Studies vary regarding the extent of amnesic properties compared to benzodiazepines.6,7 but it has recognised antiemetic and euphoric effects. Onset of action is <60 seconds (one armbrain circulation). Despite a half life of 1344 hours, duration of action is approximately 10 minutes, owing to rapid redistribution from CNS tissue to muscle and fat. Metabolic clearance equals or exceeds hepatic blood flow, suggesting extrahepatic clearance, possibly pulmonary.6 Pharmacokinetics are unaffected by renal or hepatic disease but dose reduction is required in the elderly,6 as volume of distribution falls with age.
Bassett et al19 (table 1) is a further study in the same institution following almost the same protocol. Patients were fasted for 3 hours and 10 litres of oxygen was administered routinely. At least three deviations from protocol were noted when patients were not given oxygen, and all of these patients became hypoxic.
(EMJ 2006;23(2):89)
Screening with CPK (<5000 for discontinuation) may be an effective prevention strategy (Injury, Int. J. Care Injured 45 (2014) 245–249)
Nail Polish Removers
most contain acetonitrile which is converted to cyanide in vivo.
Dystonic Reactions
buccolingual-protruding or pulling sensation of tongue
Torticollic-neck or facial spasm
Oculogyric-roving or deviated gaze
Tortipelvic-abd rigidity and pain
Opisthotonic-spasm of entire body
Give 50 mg of benadryl IV
Strychnine
seizure while awake, lift back off bed
muscle spasms
Strychnine poisoning is an unusual but dramatic poisoning in which convulsions are the major threat to life. Convulsions are predominantly at the spinal level, and the key to recognition of this poisoning is observation of convulsive activity in the awake patient without a postictal phase. Successful treatment requires aggressive airway control and treatment of seizures with benzodiazepines or barbiturates. Neuromuscular blockade may be required. Gastrointestinal decontamination is usually indicated in recent acute ingestions but may precipitate convulsions. Recovery from strychnine poisoning is usually complete and rapid if treatment is aggressive. In the absence of trauma, compartment syndrome, rhabdomyolysis, or anoxic central nervous system injury, no neurologic or musculoskeletal sequelae are expected. Confirmation of strychnine poisoning is best obtained by submitting urine or gastric aspirate for analysis utilizing a qualitative test such as thin layer chromatography (TLC).
Malignant Hyperthermia
Dextromethorphan
DXM
skittles, red hots, triple cs
presents with new-onset and otherwise unexplained psychosis. Although the authors don’t mention it, one clue to the diagnosis might be the presence of nystagmus. One other take-home lesson is that DXM will not itself show up on a urine drug screen, but in large amounts can produce a false-positive urine screen for PCP.
Reglan
Metoclopramide
Rate of Akasthisia is directly related to rate of infusion. Over 10 minute infusion sig. less side effects than 2 minute IV Bolus (EMJ 2005;22(9):621)
Toxin Induced Hyperthermia
Crit Care 2007; 11:236
Colchicine
Methotrexate
Methotrexate (MTX) is a chemotherapeutic drug that is structurally similar to folic acid. MTX inhibits dihydrofolate
reductase, an enzyme that reduces folic acid to tetrahydrofolic acid. This inhibition interferes with DNA
synthesis and cell reproduction. MTX is used in the treatment of a variety of illnesses including cancer, rheumatoid
arthritis, systemic lupus erythematosus, and psoriasis. It is given intravenously, intramuscularly, orally
and intrathecally.
Methotrexate toxicity develops due to increased patient susceptibility during treatment, excessive parenteral
or intrathecal administration, therapeutic errors by patients (e.g. taking MTX orally daily instead of weekly),
self-administration to induce abortion, or intentional oral overdoses. Clinical manifestations of toxicity include
nausea, vomiting, diarrhea, mucositis, stomatitis, esophagitis, elevated hepatic enzymes, renal failure, rash,
myelosuppression (leukopenia, pancytopenia, thrombocytopenia), acute lung injury, tachycardia, hypotension,
and neurologic dysfunction (depression, headache, seizures, motor dysfunction, stroke-like symptoms, encephalopathy,
coma). Toxic effects may occur hours to days to weeks after MTX administration or overdose.
Treatment of MTX toxicity includes the administration of activated charcoal in the event of a recent, oral overdose.
Renal failure may be prevented by adequate hydration and urinary alkalinization with sodium bicarbonate.
There are three antidotes that have been used for MTX toxicity: leucovorin, thymidine and glucarpidase.
Leucovorin (folinic acid) is the reduced and active form of folic acid. It selectively rescues normal cells from
the toxic effects caused by MTXs inhibition of the production of reduced folates. The recommended dosage in
most cases is 100 mg/m
2 intravenously every 3 to 6 hours until the plasma MTX level is less than 0.01
mcmol/L or for 3 days or longer if levels are not available. Thymidine rescues cells from the cytotoxic effects of
MTX. Its use is investigational and is only given along with other therapies. Glucarpidase (carboxypeptidase) is
an antidote that has been used recently for MTX toxicity in combination with leucovorin. It converts MTX to an
inactive form and rapidly lowers MTX blood levels. It is given as a single bolus of 50 units/kg intravenously
over 5 minutes. Leucovorin should be continued for 48 hours after glucarpidase administration. Hemodialysis
and hemoperfusion have been used to lower MTX levels. Intrathecal overdoses require special measures including
cerebrospinal fluid drainage and exchange, steroids, and antidotes. (Maryland ToxTidbits)
Dinitrophenol (DNP)
Fatal 2,4-dinitrophenol poisoning . . . coming to a hospital near you. Siegmueller C, Narasimhaish R. Emerg Med J 2010 May 29 [Epub ahead of print]
Dinitrophenol (DNP) is an industrial chemical used in the manufacture of explosives, herbicides, dyes, and wood preservatives. When ingested, DNP uncouples mitochondrial oxidative phosphorylation, interfering with the cells ability to store energy as ATP. Instead, the energy is dissipated as heat, causing severe hyperthermia that in case reports has proven very difficult if not impossible to control. In addition, the ATP depletion causes release of calcium from the sarcoplasmic reticulum in muscles. The resulting uncontrolled muscular contraction produces even more heat. Patients with DNP toxicity often die of hyperthermia, multi-organ failure, and cardiovascular collapse. Presenting signs and symptoms of acute DNP toxicity include hyperthermia, diaphoresis, nausea and vomiting, and diarrhea.
In the 1930s, DNP was often used as a diet aid after a clinical pharmacologist found that by increasing the metabolic weight controlled doses of DNP could cause an average loss of 1.5 2.0 pounds per week. One laboratory brought out a product called Formula 281, that contained DNP 1.5 grains. The promotional brochure gushed: Here, at last, is a reducing remedy that will bring you a figure men admire and women envy, without danger to your health or change in your regular mode of living. Enthusiasm for these products waned when it became apparent that the gap between the therapeutic and toxic doses was extremely narrow, and customers taking even the recommended dose started to go blind from dinitrophenol cataracts.
Unfortunately, DNP is being sold again over the internet as a weight-loss product. This fascinating case report from London describes an adult male who suicidally ingested 14×200 mg DNP tablets purchased from a website. On arrival at hospital 12 hours after ingestion, he had vomiting and diarrhea, diaphoresis, and dehydration. His pulse was 150/min, BP 104/64, respiratory rate 28.min, and temperature 38.4°C. The clinicians instituted treatment recommended by the U.K. National Poison Information Service guidelines, including fluids, cooling, and sedation. However, the patients condition deteriorated and he developed respiratory failure and an asystolic cardiac arrest from which he could not be resuscitated.
The authors make the point that the U.K. NPIS guidelines recommend treating DNP toxicity with dantrolene if the patients temperature is greater than 39-40°C. Although this is based as far as I can determine on just a single abstract, the pharmacology makes sense: dantrolene specifically inhibits calcium release from sarcoplasmic reticulum. The authors argue that the NPIS threshold for administering dantrolene may be set too high, and that giving it earlier in significant DNP toxicity may be beneficial.
Drug Stuffers and Body Packers
Mules
Review of Blood Purification
From Adv in Chronic Kidney Dis
Drug-Induced Hyperthermia
Best Review Article of Drug-Induced Hyperthermia
2,4 Dinotrophenol