cardene
can be given 1/2-1 cc at a time when diluted to 0.5 mg/ml
Systemic Hypertension
Three categories of ED presentations (Annals 41:1, April 2003; excellent review article):
- Severely Increased BP: no treatment, f/u within a week
- Hypertensive Urgency: Increased BP (DBP >115 to 120 mm Hg) with evidence of prior, but not active end organ damage. Examples are a patient with a history of MI or CVA
- Hypertensive Emergency: Increased BP with signs of acute end organ damage
JNC VII
There is no longer any category for severe increase BP.
Hypertensive urgencies and emergencies
Patients with marked BP elevations and acute target-organ damage (e.g.,
encephalopathy, myocardial infarction, unstable angina, pulmonary edema,
eclampsia, stroke, head trauma, life-threatening arterial bleeding, or aortic
dissection) require hospitalization and parenteral drug therapy.
1 Patients with
markedly elevated BP but without acute target organ damage usually do not
require hospitalization, but they should receive immediate combination oral
19
antihypertensive therapy. They should be carefully evaluated and monitored
for hypertension-induced heart and kidney damage and for identifiable causes
of hypertension. (See table 4.)
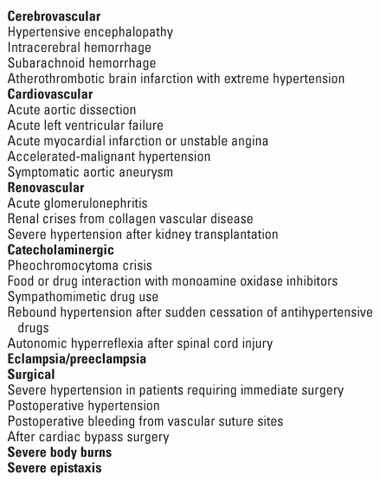
Hypertensive Crises: Emergencies and Urgencies
Hypertensive emergencies are characterized by
severe elevations in BP (>180/120 mmHg) complicated
by evidence of impending or progressive target
organ dysfunction. They require immediate
BP reduction (not necessarily to normal) to prevent
or limit target organ damage.
312,313 Examples
include hypertensive encephalopathy, intracerebral
hemorrhage, acute MI, acute left ventricular
failure with pulmonary edema, unstable angina
pectoris, dissecting aortic aneurysm, or eclampsia.
Hypertensive urgencies are those situations associated
with severe elevations in BP without progressive
target organ dysfunction. Examples include
upper levels of stage II hypertension associated
with severe headache, shortness of breath,
epistaxis, or severe anxiety. The majority of these
patients present as noncompliant or inadequately
treated hypertensive individuals, often with little
or no evidence of target organ damage.
Early triage to establish the appropriate therapeutic
strategies for these patients is critical to limiting
morbidity and mortality.
314 Patients presenting
with severe hypertension may represent as
much as 25 percent of all patient visits to busy
urban emergency rooms (ERs).
315
Patients with hypertensive emergencies should be
admitted to an intensive care unit for continuous
monitoring of BP and parenteral administration
of an appropriate agent (table 23). The initial
goal of therapy in hypertensive emergencies is to
reduce mean arterial BP by no more than 25 percent
(within minutes to 1 hour), then if stable, to
160/100110 mmHg within the next 26 hours.
Excessive falls in pressure that may precipitate
renal, cerebral, or coronary ischemia should be
avoided. For this reason, short-acting nifedipine
is no longer considered acceptable in the initial
treatment of hypertensive emergencies or urgencies.
If this level of BP is well tolerated and the
patient is clinically stable, further gradual reductions
toward a normal BP can be implemented
in the next 2448 hours. There are exceptions
to the above recommendationpatients with an
ischemic stroke in which there is no clear evidence
from clinical trials to support the use of immediate
antihypertensive treatment, patients with
aortic dissection who should have their SBP lowered
to <100 mmHg if tolerated, and patients in
whom BP is lowered to enable the use of thrombolytic
agents (see Stroke).
Some patients with hypertensive urgencies may
benefit from treatment with an oral, short-acting
agent such as captopril, labetalol, or clonidine followed
by several hours of observation. However,
there is no evidence to suggest that failure to
aggressively lower BP in the ER is associated with
any increased short-term risk to the patient who
presents with severe hypertension. Such a patient
may also benefit from adjustment in their antihypertensive
therapy, particularly the use of combination
drugs, or reinstitution of medications if
noncompliance is a problem. Most importantly,
patients should not leave the ER without a confirmed
followup visit within several days.
Unfortunately, the term urgency has led to
overly aggressive management of many patients
with severe, uncomplicated hypertension.
Aggressive dosing with intravenous drugs or even
oral agents, to rapidly lower BP is not without
risk. Oral loading doses of antihypertensive
agents can lead to cumulative effects causing
hypotension, sometimes following discharge from
the ER. Patients who continue to be noncompliant
will often return to the ER within weeks.
Causes of hypertensive crises Abrupt increase in BP in patients with chronic hypertension Renovascular hypertension/renal disease Withdrawal from antihypertensive drugs Drug-induced hypertension (eg, amphetamines, diet pills, tricyclic antidepressants, street drugs [eg, cocaine]), drug withdrawal, pheochromocytoma Preeclampsia/eclampsia Head injury of any kind Vasculitis Scleroderma and other collagen-vascular diseases
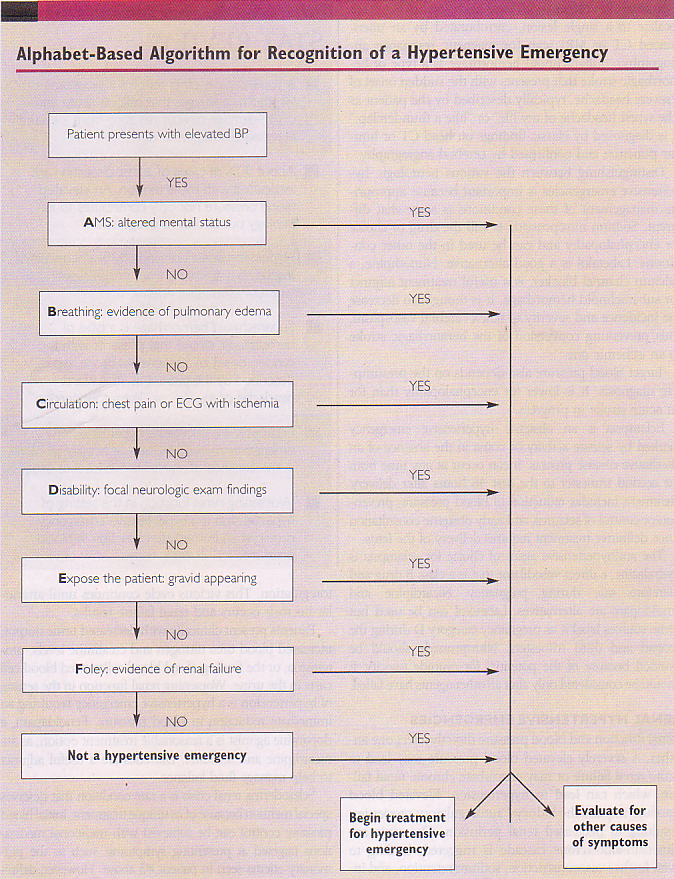
Clinical Examination
The blood pressure at triage does not correlate with bps taken under AHA reference conditions (Academic Emergency Medicine Volume 11, Number 3 237-243)
Take BP in both arms, and before and after evaluation to get true reading
Examine fundi for retinal hemorrhage and papilledema
Signs of Heart Failure
Creatinine and UA for protein and blood. Urine dipstick totally normal rules out clinically significant creatnine elevation (AEM 2002 9:1) Signs of acute damage are large numbers of red cells and red cell casts
unfortunately 2nd study showed 82% sends 34% spec (Am J Emerg Med. 2010 Jun;28(5):613-6)
EKG
Numbers don’t matter, only whether there is end-organ damage or not (Journal of Hypertension Issue: Volume 30(5), May 2012, p 882–883)
Testing
Screening tests probabl are very low yield (Ann Emerg Med 2008;51:231)


Precipitious Drops in BP
patients prescribed short-acting nifedipine (which result sin precipitious drops in BP) had a much higher stroke rate (Neurology 2011;77:1229–1234)
Drugs for HTN Emergency
nitroprusside is the traditional first choice (beware in renal and liver failure), but labetalol is quickly becoming a more attractive option. Aim to reduce MAP by 30-40% over the first two hours.

Labetalol
Labetalol is more potent at beta that at alpha 1 adrenoceptors in man; the ratio of beta-alpha antagonism is 3:1 after oral and 6.9:1 after intravenous administration. (Pharmacotherapy. 1983 Jul-Aug;3(4):193-219.)
Nicardipine
Start 5 mg/hr (50 cc/hr)
Increase infusion by 2.5 mg/hr (25 cc/hr)
Dosage should not exceed 15 mg/hr (150 cc/hr)
For rapid control, change every 5 minutes
For gradual control, change every 15 minutes
For rapid control, decrease rate to 3 mg/hr (30 cc/hr)
For gradual control, maintain current infusion rate
Clue RCT nicardipine vs. labetalol (Crit Care 2011;15:R157)
more likely to reach goal < 30 min
Nitroprusside
cyanide is converted to thiocyanate in the liver using substrate of thiosulfate
increased anion gap acidosis is late sign of toxicity
treat with thiosulfate or hydroxocobalamin
Cerebrovascular Emergencies
Autoregulation of cerebral blood flow is altered in patients with hypertension particularly in the setting of underlying cerebrovascular disease such that even slight decreases in blood pressure increase the risk of a cerebral ischemic event. The National Institute of Neurologic Disorders and Stroke (NINDS) recommends deferral of treatment of systolic pressures of 185-220mm Hg and/or diastolic pressures of 105-120mm Hg in the absence of other clear indications for immediate intervention. (J Emerg Med 19(4):339, 2000)
AHA recommendations for hemorrhagic stroke is to treat MAP>130 or SBP> 220. Nimodipine is to prevent vasospasm not to treat the BP.
Accelerated-Malignant Hypertension
Most commonly occurs in young black males with renal parenchymal disease or renovascular disease. Ocular findings will be present on fundoscopic exam. Papilledema is the sine qua non of malignant hypertension. If it is absent, then it is accelerated hypertension, but the prognosis is just as bad. Treatment should begin immediately.
Hypertensive Encephalopathy
Triad of htn, altered mental status and papilledema (often) heralds this condition. This state is most likely to occur in previously normotensive patients whose cerebral autoregulatory system is not prepared for the precipitous rise in BP. A CT scan will show characteristic changes.
Secondary Hypertension
Acute Renal Disease
Renal Artery Stenosis-young white women get medial fibroplasia of renal arteries. Can also be seen in blacks and whites often with rapidly progressive disease. ACEI may cause improvement with unilateral stenosis, but failure in bilat.
Glomerulonephritis-IgA (#1 cause), post-Strep, Henoch-Schoenlein Purpura
Scleroderma-Induced Renovascular Hypertension
will have elevated renin
need to give high dose ACEIs
Preeclampsia
From 20 weeks gestation till 2 weeks postpartum
Toxicologic Ingestions
sympathomimetics, MAO interactions
Coarctation of the Aorta
Pheochromocytoma
Tachy, HA, hypertension, check urine metanephrine, serum catecholamines
Give IV phentolamine
associated with neurofibromatosis
Although measurement of plasma free metanephrine levels has been recently advocated by some groups, 24-hour urinary catecholamine levels and total metanephrine level have consistently proven to be the most specific tests available for the diagnosis of phaeochromocytoma.5,10 Elevations in the level of one or more of these analytes (above the 95% reference range designated as the upper limit of normal by laboratories) are common in patients with paroxysmal symptoms or poorly controlled hypertension not due to phaeochromocytoma. Thus, we recommend that higher cut-off values, roughly two times the upper limit of normal for most laboratories, be used to identify patients suitable for further workup. Repeat biochemical testing 6 weeks after stopping drugs likely to confound the results is ideal, and tests performed during major physical or psychological stress should be interpreted with extreme caution (if performed at all). It is important to note that alterations in plasma catecholamine levels may be caused not only by medications, but also by the underlying diseases being treated (eg, major depression in the case of tricyclic antidepressants or severe heart disease in the case of β-blockers).11-13 All patients should undergo at least two 24-hour urine collections for measuring levels of catecholamines and their metabolites. Clonidine suppression testing the measurement of plasma free normetanephrine before and after the oral administration of 0.3 mg clonidine is highly sensitive and specific, and may be a useful adjunct in patients with more than one prior set of equivocal tests.6 (eMJA)
Medications and conditions that may cause false positive results of biochemical tests for phaeochromocytoma
Medication or condition
Test(s) confounded
Tricyclic antidepressants
Urinary catecholamines and metanephrines, plasma free metanephrines
Clozapine
Urinary catecholamines and metanephrines
Phenoxybenzamine
Plasma free metanephrines
Calcium channel blockers
Plasma noradrenaline, urinary noradrenaline, urinary adrenaline
β-adrenergic blockers
Urinary catecholamines and metanephrines, plasma free metanephrines (minor effect)
α1-adrenergic blockers
Urinary noradrenaline
Sympathomimetics
Urinary catecholamines and metanephrines, plasma free metanephrines
Buspirone
Urinary metanephrines
Major physical or psychological stress*
Urinary catecholamines and metanephrines, plasma free metanephrines
* Hypoglycaemia, hypoxia, hypovolaemia, stroke, surgery, myocardial infarction, heart failure, severe pain, depression, panic disorder, sleep apnoea.
Hyperaldosteronism
Draw tube for renin and aldosterone
Withdrawal
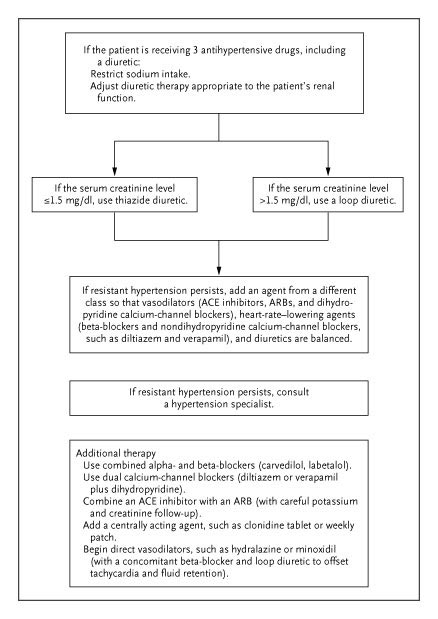
Outpatient Treatment
NIH’s ALLHAT study shows equal effectiveness between thiazide diuretic (chlorthalidone), lisinopril, and amlodipine for the prevention of MIs and coronary death. The diuretic was more effective at preventing heart failure and more effective than amlodipine at preventing stroke. The ALLHAT study included more minorities than a recent Australian study which showed ACEI are better. Probably the best choice is an ACEI and a diuretic for double therapy in all comers.
Antihypertensive Agents
Loop Diuretics
furosemide (1) to bumetanide (40) to torsemide (4)
synergistic increase in auditory toxicity of aminoglycosides
electrolyte disturbances
NSAIDS reduce efficacy by blocking prostaglandin synthesis
Thiazides
Can precipitate or exacerbate hyperglycemia in diabetics and prediabetics
ACEI
captopril is solely cleared by kidneys
Iron supplementation inhibits cough associated withACE inhibitors. (Hypertension. 2001 Aug;38(2):166-70.)
There is a lack of relationship between symptoms and hypertension (Am J Emerg Med 2005;23(2):106)
ACEP Clinical Policy
Patient Management Recommendations: Do asymptomatic patients with elevated blood pressures benefit from rapid lowering of their blood pressure? Level A recommendations None specified. Level B recommendations 1 Initiating treatment for asymptomatic hypertension in the ED is not necessary when patients have follow-up. 2 Rapidly lowering blood pressure in asymptomatic patients in the ED is unnecessary and may be harmful in some patients. 3 When ED treatment for asymptomatic hypertension is initiated, blood pressure management should attempt to gradually lower blood pressure and should not be expected to be normalized during the initial ED visit. Level C recommendations None specified. Annals of Emergency Medicine Volume 47, Issue 3 , March 2006, Pages 237-249
Once these are considered and ruled out, management should include fluid replacement with normal saline and blood pressure reduction. Why the former? Hypertensive emergencies cause a pressure induced natriuresis by increasing the forces exerted on the renal afferent arterioles. The increased pressure activates the rennin/angiotensin/aldosterone system, causing diuresis and volume depletion, which can be easily corrected. Administration of saline may cause a decrease in blood pressure by itself before institution of blood pressure lowering medication. Pressure reduction should aim for a 25% reduction in the first two hours, 15% in the first, and 10% in the second. But dont overshoot! A 40% reduction in blood pressure will lead to its own neurologic event. Use titratable meds only to achieve the lowered pressure. Sublingual, transdermal, and oral meds can cause a precipitous decline and cant be reversed.
Headache
Headache in patients with mild to moderate hypertension is generally not associated with simultaneous blood pressure elevation Abstract Objective: Although headache is regarded a symptom of hypertension, its relation to blood pressure, especially in mild and moderate hypertension, is not clear. Thus, the aim of the study was to investigate whether headache in patients with mild to moderate hypertension may be attributed to simultaneous elevations in blood pressure.Design and methods: Ambulatory blood pressure monitoring (ABPM) was performed in patients (mean age 48 ± 10 years, n = 150, 92 men, 58 women) classified, according to their office blood pressure, as stage 1-2 hypertensives (JNC VI). Headache periods were recorded in patients’ diaries. Results: Headaches were generally not directly associated with blood pressure elevations in the studied group of stage 1-2 hypertensive patients because (i) blood pressure values from headache periods were not significantly higher than those from headache-free periods; (ii) blood pressure values directly preceding the pain were not significantly different from values at the beginning of headache; and (iii) in the vast majority of hypertensives, their maximal blood pressure values were recorded during headache-free periods. Moreover, in some instances, patients who showed maximal ABPM values during headache had relatively high blood pressure, i.e. 180/110 mmHg.Conclusions: Our results did not support the opinion that headache experienced by stage 1-2 hypertensives was generally caused by simultaneous elevation in blood pressure. The direct mechanisms of headache in hypertension, as well as the relation between increments in blood pressure above 180/110 mmHg and headache, need further investigations.
From Renal Fellow Network
Secondary forms of hypertension
Lisa Cohen recently summarized rare “genetic” forms of hypertension including Liddle’s syndrome and PHA type II (Gordon’s syndrome).
I want to summarize other causes of “secondary” hypertension which are not inherited (at least not typically in a Mendelian transmission) and which are potentially “fixable”. These phenotypes are distinct from primary hypertension which affects the vast majority of our patients. Secondary forms of hypertension affect typically less then <5% of patients with hypertension.
In order to identify a reversible cause for hypertension following data needs to be obtained:
- HPI
- Family history
- Physical exam
- Initial labs including Chem7, Lipid panel, Urine analysis, EKG
- Indications for further labs include abnormal initial tests (high Ca++ levels, low K+ levels), abrupt onset of hypertension, young age (<30),>50), hypertension resistant or refractory to 3+ medications, worsening hypertension in a previously well controlled patient, BP >180/110 at onset.
The most common forms of secondary hypertension are:
- Renovascular hypertension
- Coarctation of aorta
- Cushings syndrome
- Primary Aldosteronism
- Thyroid/parathyroid disease
- Pheochromocytoma
Typically others causes such as CKD or sleep apnea are not considered “secondary” forms of hypertension. Physical and laboratory findings can help and guide in ruling out secondary forms of hypertension: If you find this -> think this !!!
- Truncal obesity and striae -> Cushing’s syndrome
- Labile hypertension -> Pheochromocytoma
- Abdominal bruits -> renovascular hypertension
- Decreased BP and Pulse in lower extremities -> Coarctation of aorta
- Abdominal flank masses -> Polycystic kidney disease
- Elevated Crea and/or abnormal UA -> parenchymal kidney disease
- Hypercalcemia -> Hyperparathyrodism
- Hypokalemia -> Hyperaldosteronism (also Cushing’s syndrome and Pheochromocytoma can present with this).
Last but not least, a few more facts on the three most common secondary forms of hypertension:
- Renovascular hypertension- Renal artery artherosclerosis (males>50, Fibromuscular dysplasia (females<40),Other (rarer) causes include vasculitis, scleroderma, Takayasu arteritis, etc. – Labs show typically hypokalemia and hyper-reninemic hyperaldosteronism – Screening tests recommended are Doppler US, MRA, CT angio, captopril renogram – Gold standard is arteriography which could show string of beads vs. single stenosis
- Hyperaldosteronism: Aldo causes increased Na+ uptake in distal tubule -> increase in intravascular volume
-Suspect in patients with unexplained low K+
-Main causes are adrenal adenomas (~ 70%) and b/l adrenal hyperplasia (~ 25%)
-Screening by checking stimulated PRA or PRC which will be undectable or low
-Confirm screening tests with salt/fluid loading -> “elevated” Aldo level will NOT be suppressed - Pheochromocytoma:
-Rare tumors arising from chromaffin tissue of the adrenal gland
-90% occur in the adrenal medulla
-10% are b/l, 10% are malignant and 10% are familial!
-Associated with MEN II
-Remember that 33-50% of patients have sustained hypertension !
-Suspect it if refractory to treatment
-Screen for serum or urine metanephrines
-CT adrenals or/and MIBG scan (meta-iodo-benzyl-guanidine) to detect tumors
transdermal GTN (5 mg) or control lowered peripheral systolic BP by (mean) 23 mm Hg (95% CI, 2 to 45; (Hypertension. 2006;47:1209-1215.)