Delerium vs. Dementia-time course, autonomic involvement, and acuity
Delerium-think medications, esp. anti-ach also consider withdrawal
DTs-3 to 5 days, Withdrawl seizures-can start within 6 hours
If need to sedate use Haldol and Ativan combo
Pseudodementia-from depression in the elderly
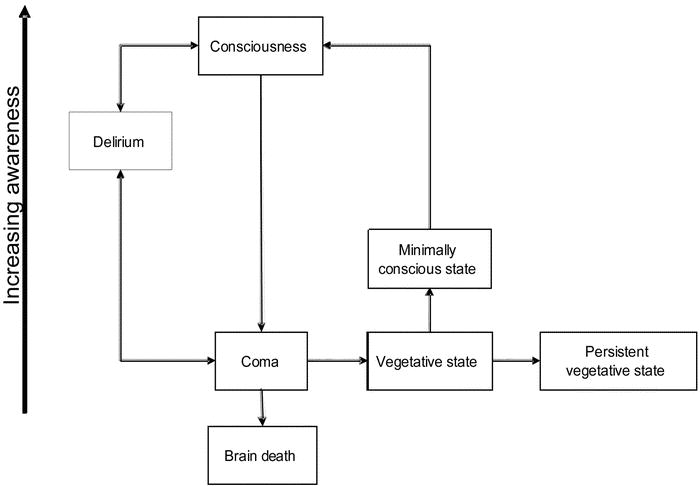
Decreased LOC
Acute focal neurologic deficit
Decreased Level of Attention
Delirium
The term delirium stems from the Latin word delirare. In common usage it meant to be crazy and was derived from two other Latin words, de and lira (the ridge between furrows). The literal translation is to go out of the furrow while plowing.12 In the first century AD, Celsus used the term delirium to distinguish a constellation of symptoms from that of hysteria, depression, and mania.13 It corresponded to phrenitis (English derivativefrenzy), which was known to Hippocrates (460-366 BC), who observed the appearance of cognitive and sleep disturbances and agitated behavior in patients with febrile illnesses.
DSM-IV include:1
1. Disturbance of consciousness (i.e., reduced clarity of awareness of the environment) with reduced ability to focus, sustain, or shift attention;
2. A change in cognition (e.g., memory deficit, disorientation, language disturbance) or the development of a perceptual disturbance that is not accounted for better by a pre-existing, established, or evolving dementia;
3. The disturbance develops during a short period (usually hours to days) and tends to fluctuate during the course of the day. There is evidence from the history, physical examination, or laboratory findings that the disturbance is caused by the direct physiologic consequences of a general medical condition, substance intoxication or side effect, substance withdrawal, multiple factors, or unidentified etiology. For substance intoxication, side effects, or withdrawal, there must be a temporal or etiologic relationship to the disturbance.
Quick Confusion Scale (QCS).


CAM

Differential DX
Drugs and withdrawal
Endocrine (thyroid, Addison’s)
Lungs (hypercapnia, pneumonia)/Lytes (hypoglycemia)
Infection
Restraints, reduced mobility
Intracranial
Uremia/retention
Myocardial
CBC, LFTS, Lytes, Pulse Ox, ECG (Consider Enzymes), C-XR, UA, and ammonia levels
death after excited/agitated delerium (AJEM 2001;19:187)
Coma and Depressed Level of Consciousness
Arousal takes place in the brainstem in the ascending reticular activating system (RAS) and the cerebellum
GCS-eyes 4 verbal 5 motor 6
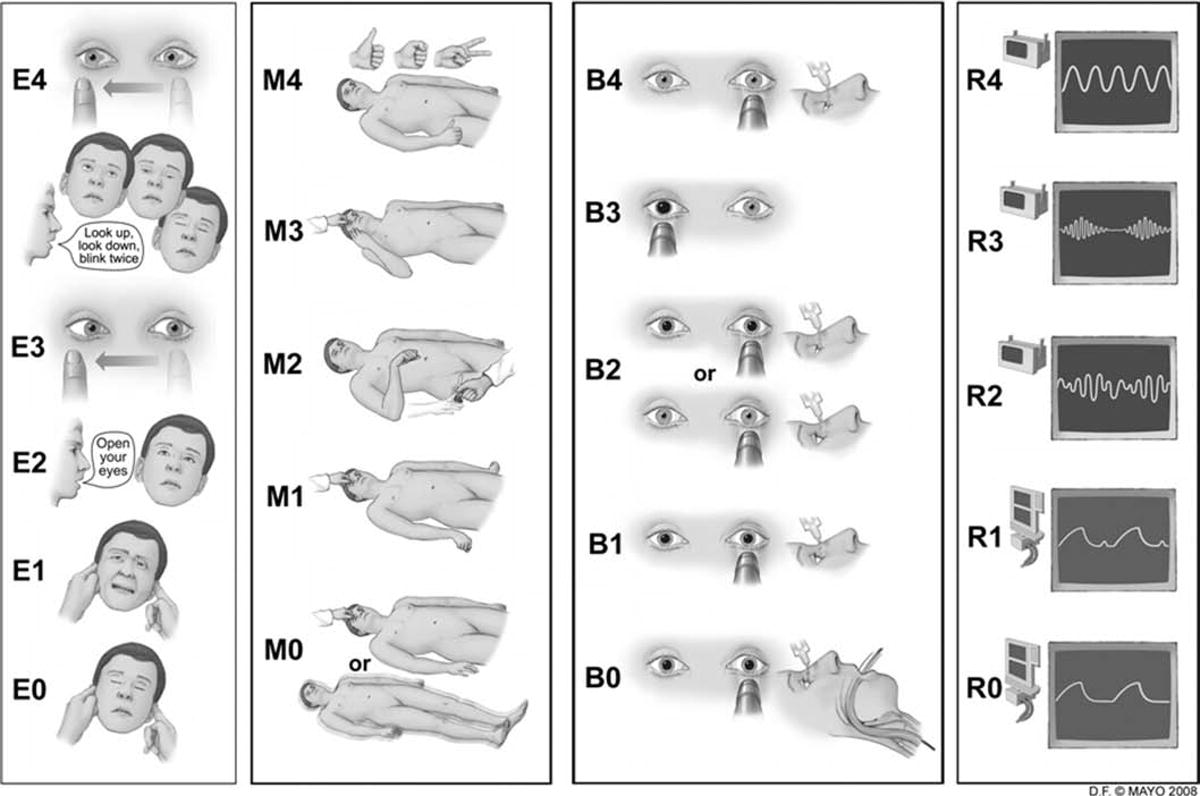
FOUR Score
(Critical Care Medicine Issue: Volume 40(9), September 2012, p 2671–2676)
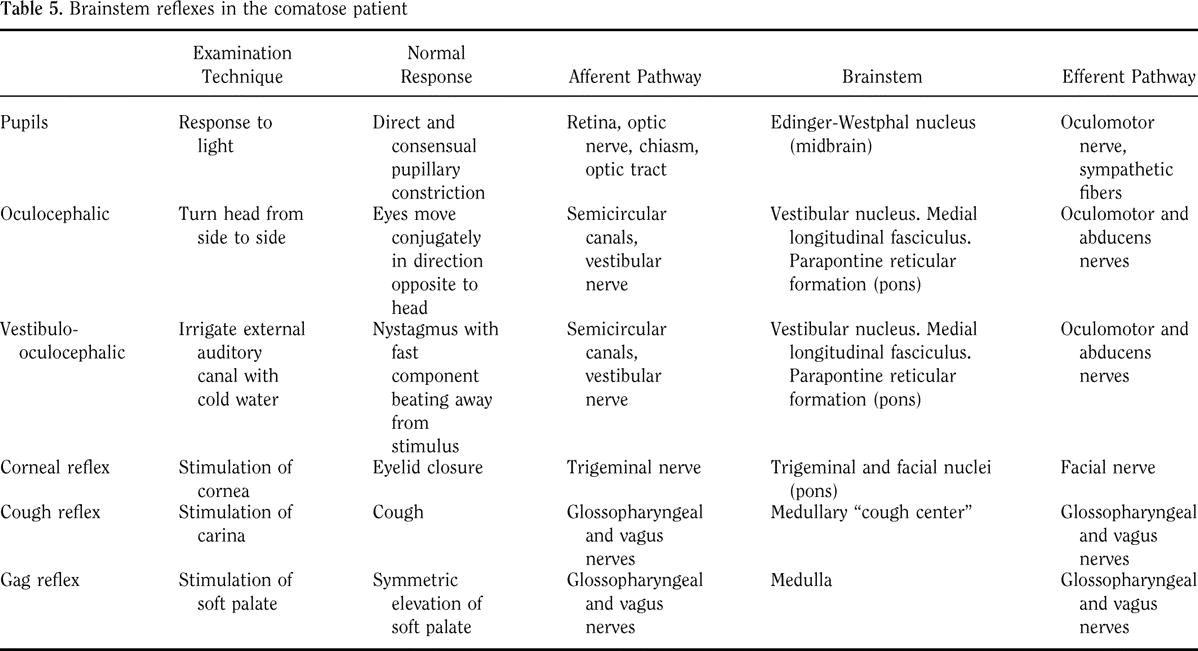
Neuro Exam in the Comatose Patient
Triple flexion-flexion of the hip, knee, ankle. Spinal cord reflex, does not imply any higher functioning.
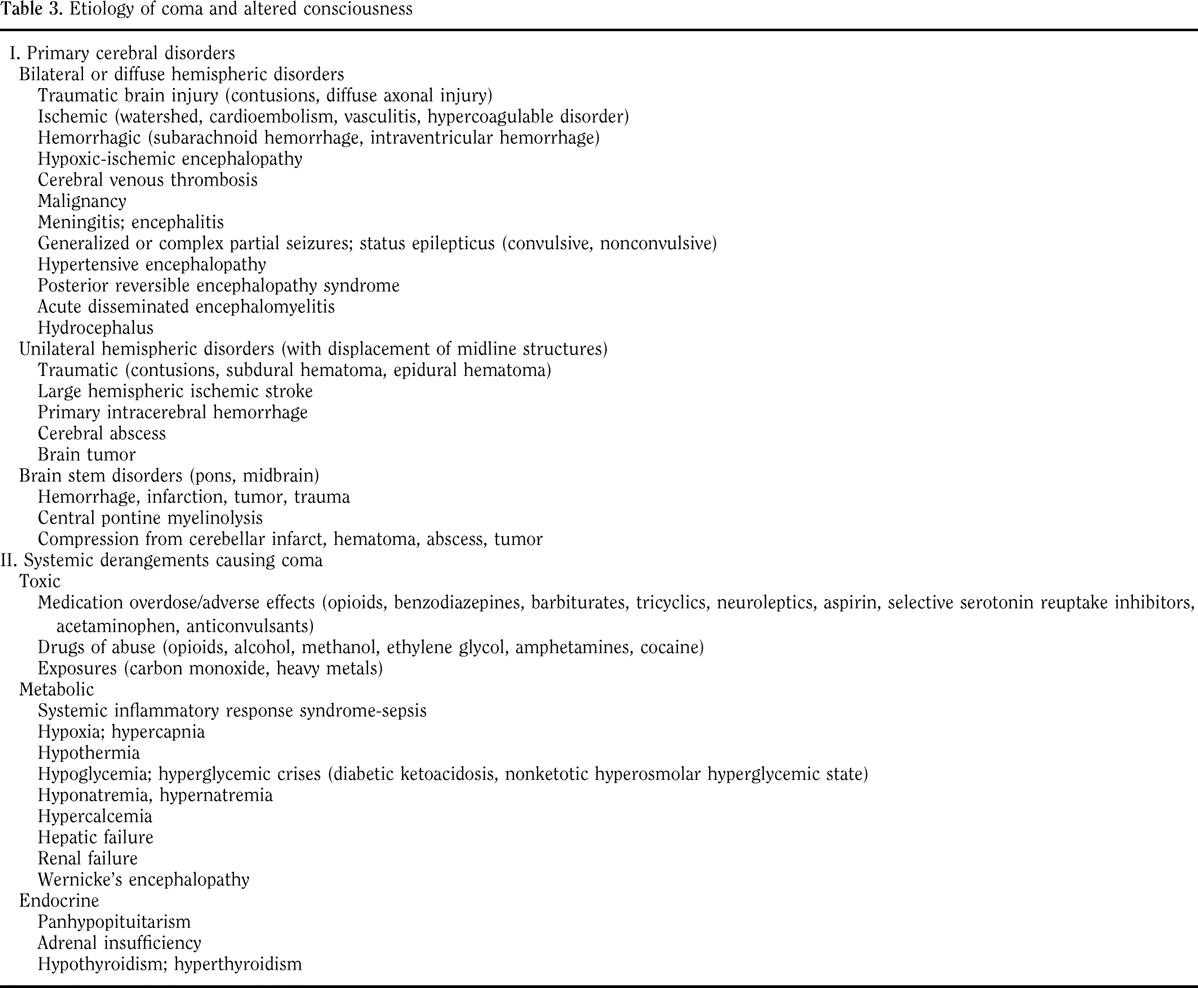
Etiology of Coma
- Diffuse Brain Dysfunction
- Neuronal damage caused by deprivation of oxygen, glucose, or metabolic cofactor
- Hypoxia with an intact CBF, severe pulmonary disease, anemia
- Decreased CBF (e.g., postcardiac arrest, cardiogenic and hypovolemic shock)
- Cellular toxins: carbon monoxide, cyanide, hydrogen sulfide
- Hypoglycemia
- Thiamine deficiency (Wernicke-Korsakoff syndrome)
- Endogenous CNS toxins
- Hyperammonemia (hepatic coma, postureterosigmoidostomy, prune belly syndrome)
- Uremia
- CO2 narcosis
- Hyperglycemia
- Exogenous CNS toxins
- Alcohols: ethanol, isopropyl alcohol
- Acid poisons (methanol, ethylene glycol, salicylates)
- Sedatives and narcotics
- Anticonvulsants
- Psychotropics
- Isoniazid
- Heavy metals
- Endocrine disorders
- Myxedema coma, thyrotoxicosis
- Addisons disease, Cushings disease, pheochromocytoma
- Abnormalities of ionic environment of CNS
- Hyponatremia, hypernatremia
- Hypocalcemia, hypercalcemia
- Hypomagnesemia, hypermagnesemia
- Hypophosphatemia
- Acidosis, alkalosis
- Environmental disorders and disordered temperature regulation
- Hypothermia
- Heat stroke
- Neuroleptic malignant syndrome
- Malignant hyperthermia
- Intracranial hypertension
- Hypertensive encephalopathy
- Pseudotumor Cerebri
- CNS inflammation or infiltration
- Meningitis
- Encephalitis
- Encephalopathy
- Cerebral vasculitis
- Subarachnoid hemorrhage
- Carcinoid meningitis
- Traumatic axonal shear injury
- Primary neuronal or glial disorders
- Creutzfeldt-Jakob disease
- Marchiafava-Bignami disease
- Adrenoleukodystrophy
- Gliomatosis cerebri
- Progressive multifocal leukoencephalopathy
- Seizures and postictal state
- Focal Lesions of the CNS
- Supratentorial lesions
- Hemorrhage (traumatic and nontraumatic)
- Intracerebral
- Epidural
- Subdural
- Pituitary apoplexy
- Infarction
- Thrombotic arterial occlusion
- Embolic arterial occlusion
- Venous occlusion
- Tumors
- Abscess
- Hemorrhage (traumatic and nontraumatic)
- Subtentorial lesions
- Compressive
- Cerebellar hemorrhage
- Posterior fossa subdural or extradural hemorrhage
- Cerebellar infarct
- Cerebellar tumor
- Cerebellar abscess
- Basilar aneurysm
- Destructive
- Pontine hemorrhage
- Brainstem infarct
- Basilar migraine
- Brainstem demyelination
- Compressive
- Supratentorial lesions
Q1. Whats the differential for the decreased level of consciousness? (From LitFL Blog)
There are many ways to break this down into a logical sieve. This is a modified version of the apporach described by Bala Venkatesh in Ohs Intensive Care Manual:
Differential Diagnosis of Coma
Category Specific Disorder Clinical features Key investigation Focal signsCVA:
- Ischemic
- Haemorrhagic
Risk factors for CVA CT Trauma Look signs of base-of-skull fracture CT Space occupying lesion:
- Infective
- non-infective
Look for ENT and dental sources of infection Past history of cancerImmunosuppression CT Meningism Meningitis ormenigoencephalitis FeverMeningococcal rash LPCT Sub-arachnoid haemorrhage Worst headache everSubhyaloid hemorrhages SAH risk factors LPCT No focal signs or meningism
(MESOT)
Metabolic causes:
- Hypoxia
- Hypercapnoea
- Hyponatraemia
- Hyperglycaemia
- Hypoglycaemia
- Hypo/hyperthermia
- Hypo/hyperosmolarity
History essential SO2ABGETCO2UECBSLTemperature ketones Endocrine:
- Adrenal insufficiency
- Hypopituitarism
- Hypothyroidism
- Diabetic coma
Time courseSteroid medicationsPhenotype TFTfree T3/4TemperatureBSLUEC Ca, PTHCortisol Seizures (including eclampsia) ?witnessed?post-ictal?non-convulsive epilepsy EEGCT for SOL Organ Failure
- Renal: uraemia
- Liver: PSE
Urine outputHistory/exam findings of liver disease? paracetamol OD EUCLFTs, NH3INR Toxins/drugs, especially:
- Sedatives
- Narcotics
- Alcohol
- Psychotropics
- Carbon monoxide
- Many other poisons!
Toxicology risk assessment ABG analysisSpecific drug levelsOsmolality ECG Pseudocoma history of mental illnesshistory of sleep disorder Diagnosis of exclusion
This, of course, is a very generic approach. Immediately post op, you can also think of causes as being:
- Related to the anaesthetic
- Related to the surgery
- Related to post-operative events
Again, an approach modified from that of Bala Venkatesh in Ohs Intensive Care Manual is shown::
Pupillary abnormality Cause Pathology Miosis (<2mm)Unilateral Horners SyndromeLocal pathology/ trauma Sympathetic paralysisDamage to sympathetics Bilateral Pontine lesionThalamic haemorrhageMetabolic encephalopathySenile miosisArgyll-Robertson pupils Holmes-Adie pupilsDrug ingestion, eg.
- Organophosphate
- Barbiturate
- Narcotics
Sympathetic paralysis
Mechanisms:
- Cholinesterase inhibition
- Central effects
Mydriasis (>5mm)Unilateral Uncal herniationMidbrain lesion CN3 stretched on petroclinoid ligamentCN3 nucleus damage Bilateral fixed pupils Bilat uncal herniationMassive midbrain bleed Hypoxic injuryDrugs:
- Atropine
- Tricyclics
- Sympathomimetics
Brain herniationBilateral CN3 damage Mesencephalic damageMechanisms:
- Parasympathetic paralysis
- TCAs pevent reuptake of catecholamines by nerve endings
- Sympathetic stimulation
For further review read Neurological Mind-boggler 002 on the causes of coma with small pupils, and Ophthalmological Befuddler 001 for the causes of a dilated pupil.
The false-localizing ipsilateral hemiparesis,resulting from compression of the crus cerebri by the tentorium,likewise became known as the KernohanWoltman syndromeor Kernohan’s notch phenomenon (Figure 1A). Although originallydescribed in a patient with a primary brain tumour, the phenomenonmay also occur with traumatic brain injury or with displacementof the cerebral peduncles
 Figure 1: (A) Schematic coronal section of the brain showing large (supratentorial) right subdural hematoma causing ipsilateral transtentorial herniation, which has resulted in compression of the contralateral cerebral peduncle (broken, red arrow). This led to ipsilateral (right-sided) weakness. (B) Schematic coronal section of the brain showing (infratentorial) right meningioma (M) causing upward and leftward displacement of the midbrain and cerebral peduncles, which has resulted in compression of the left cerebral peduncle and corticospinal tracts against the tentorium cerebelli (open arrow), which contributed to the ipsilateral (right-side) weakness. In both figures, the solid arrows indicate the direction of shift due to the mass effect, either from the subdural hematoma or from the tumour.
Figure 1: (A) Schematic coronal section of the brain showing large (supratentorial) right subdural hematoma causing ipsilateral transtentorial herniation, which has resulted in compression of the contralateral cerebral peduncle (broken, red arrow). This led to ipsilateral (right-sided) weakness. (B) Schematic coronal section of the brain showing (infratentorial) right meningioma (M) causing upward and leftward displacement of the midbrain and cerebral peduncles, which has resulted in compression of the left cerebral peduncle and corticospinal tracts against the tentorium cerebelli (open arrow), which contributed to the ipsilateral (right-side) weakness. In both figures, the solid arrows indicate the direction of shift due to the mass effect, either from the subdural hematoma or from the tumour.
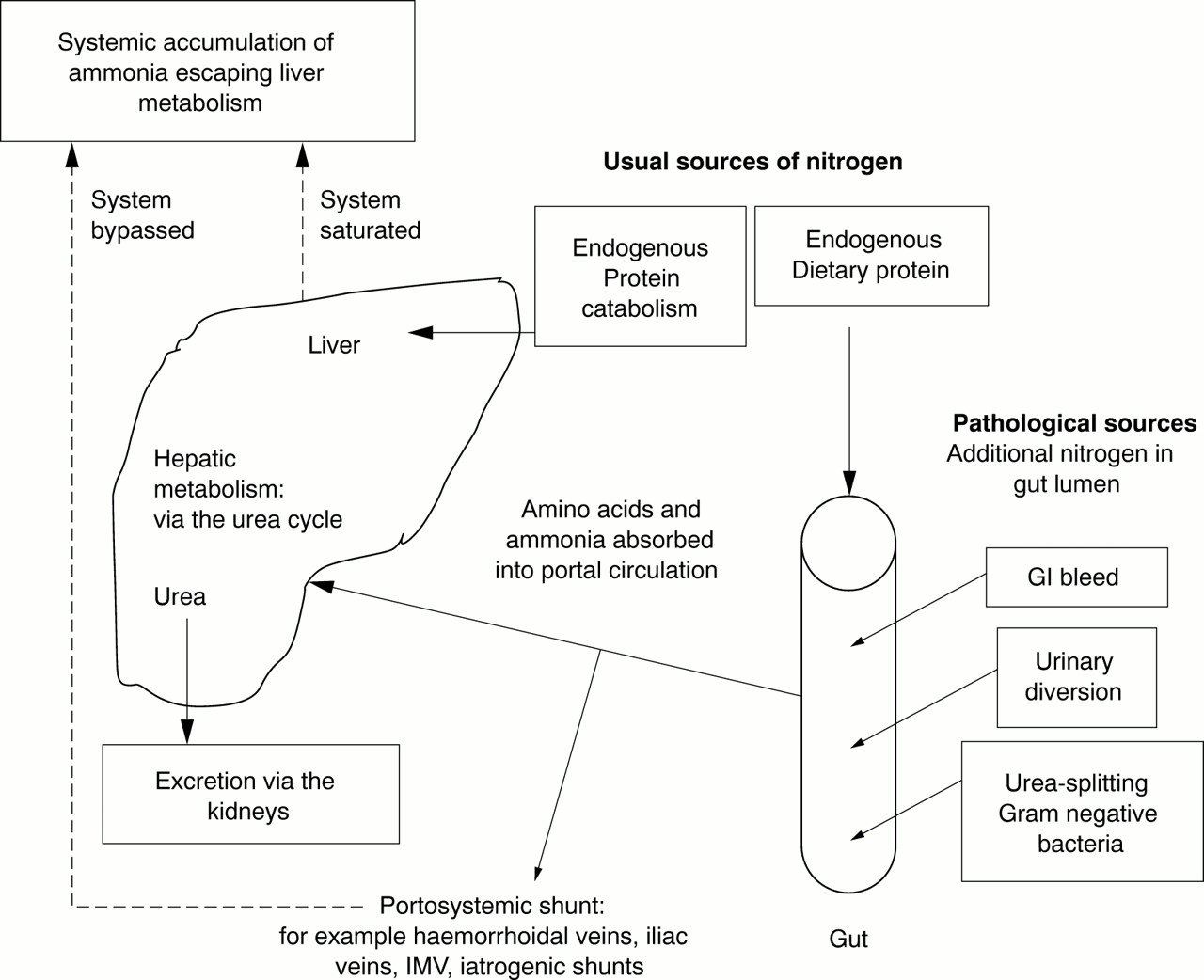
Hyperammonemia
can be non-hepatic
(Postgrad Med J 2001;77:717)
can be from massive gi bleeding resulting in absorbtion of large amounts of nitrogen
Causes of non-hepatic hyperammonaemia
Inherited defects of the urea cycle enzymes Portosystemic shunts Transport defects of intermediates in the urea cycle Urinary Organic acidurias Urinary diversion for example, ureterosigmoidostomy and ileal conduit Other metabolic causes Urinary tract infections Hyperinsulinaemic hypoglycaemia Subureteric injection for vesicoureteric reflux Distal renal tubular acidosis Haematological Primary carnitine deficiency Following allogenic peripheral blood progenitor cell transplantation Fatty acid oxidation defects Multiple myeloma Drugs Acute myeloblastic leukaemia, chronic myelocytic leukaemia Chemotherapyfor example, 5-fluorouracil, asparaginase Other Sodium valproate Parenteral nutrition Anaesthetic agentsfor example, halothane, enflurane Muscular origin Reye’s syndrome* Idiopathic * Need to exclude inborn errors of metabolism as possible causefor example, medium chain acyl-CoA deficiency. With normal liver function, as distinct from portosystemic shunts occurring in the context of chronic liver disease where resultant hyperammonaemia may be termed hepatic hyperammonaemia
Reversible Posterior Leukoencephalopathy Syndrome (RPLS) or (PRES)
encephalopathy
aka posterior reversible encephalopathy syndrome (PRES)
not always reversible or confined to posterior
vasogenic edema on MRI primarily in the posterior brain
presents c HA, confusion, visual sx, and seizures
Coma with Pinpoint Pupils
from life in the fast lane
The differential diagnosis of coma with small pupils includes:
Non-toxicological causes
- Pontine lesions (infarct or hemorrhage)classically involves sudden collapse with coma, pinpoint pupils and a spastic tetraparesis with brisk reflexes.
- Bilateral Horners syndrome*central (e.g. massive thalamic or supra-thalamic lesions, lateral brainstem lesions), pre-ganglionic (e.g Pancoast tumour), post-ganglionic (e.g. neck trauma, carotid artery dissection, cluster headaches)
- Senile miosis*
- Argyll-Robertson pupils*small, irregular, fixed pupil with little response to atropine and acts like a prostitute accommodates but doesnt react to light.nearly pathognomonic of neurosyphillis
- Pseudo-Argyll Robinson pupils* (more likely to be mid-sized) diabetes mellitusany chronic lesion of the rostral midbrain (e.g. multiple sclerosis, encephalitis, Lyme disease, pinealoma, syringobulbia, chronic alcoholism)
- Holmes-Adie pupils* (constrictive phase)
Toxicological causes
- Sedatives
opioidsclonidinebarbiturateschloral hydrateGHB
- Antipsychotics
phenothiazines (eg. chlorpromazaine)atypicals (olanzepine, quetiapine, clozapine)
- Cholinergic agents
acetylcholinesterase inhibitors organophosphatescarbamatesnerve agents (e.g. sarin) Alzheimers dementia agents* e.g. donezepil, tacrineMyasthenia gravis agents* eostigmine, physostigmine, edrophonium Acetylcholine agonists muscarinic agents pilocarpine (eye drops)*nicotinemushrooms
- Other drugs
valproatephenoxybenzamine (alpha blocker) beta blocker eye drops*
| | |