Esophagus has no serosa
Foreign Body/Food Bolus in Esophagus
Will orient coronal in esophagus and sagittal in the trachea,
Try glucagon and SL nitroglycerin.
If pill lodged in the esophagus, give sucralfate on empty stomach without antacids
The average transit time for the cricopharyngeus is to the stomach is between three and five seconds.
Get AP and lateral of the neck and chest and abdominal films. Every symptomatic patient should get endoscopy.
Glucagon 1 mg IV
Almost always from underlying pathology so get patient scoped, as outpatient if bolus moves
Glucagon to relax esophagus along c carbonated beverage if foreign body
No reason to think this is effective (Emerg Med J-2015-Best Evidence Topic Reports-85-8)
When plain radiography is used, residual pneumoperitoneum commonly persists for 2 -3 days following surgery, including laparoscopic surgery. It resolves in approximately 95% of patients by day seven. CT scanning, as might be expected, is much more sensitive, and has been noted to detect free air up to 18 days following surgery (EMEDhome.com)
Airway-Café Coronary
Get X-Rays, if sample of object available, place on shoulder for comparison
On AP-Trachea-coin is sag, esophagus is coronal
If bronchial obstruction, lungs will be expanded on exp film, if complete will be ateletatic on exp film
Esophageal objects-should be removed, can try glucagon
GI-consider golytely
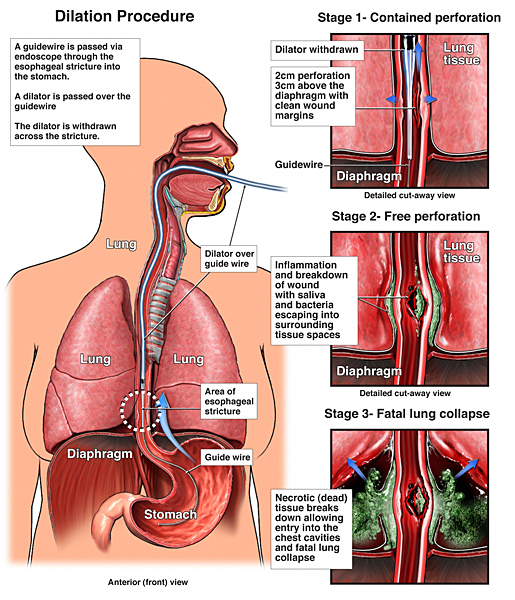
Esophageal Perforation/Rupture (Booerhave’s)
Left Posterio-lateral portion of esophagus gives left effusion/hemothroax/pneumothorax/pneumomediastinum
First off, if you suspect or desire to “know” then gastrograffin is CONTRAINDICATED. The false negative rate of gastrograffin is legend. The papers to support the desire of radiology to use gastrograffin simply does not exist. If there is an injury to the esophagus, you want to know it, and should use barium. If barium leaks, you are going to be in the chest and clean it out almost immediately anyway. If aspirated during the test, gastrograffin is very toxic to the lungs, whereas barium is not.
perforations in the neck and upper mediastinum are repaired and drained in the neck. Perforations in the chest go to the left side for low leaks in the right side for high leaks must cover muscle flap and have the floppy shrinkage
spontaneous perforation results from a conscious attempt to prevent vomiting the esophagus blows at the weakest point, usually located just above the lower esophageal sphincter.
Gun shot wounds to the chest will hit the esophagus in about one in 20 cases .disruption of the esophagus implies a violent deceleration, though intrusion of osteophytes can occur at a lower degree of violence
If sepsis has already delete set in the best course, is performance of an esophagectomy and provide wide drainage. You can restore continuity at a time of your choice.
In severe caustic injuries, the only real choice is an emergency resection,

one center’s experience with aggressive conservative treatment. Drainage with continuous checking and redrainage of any leaks (Ann Surg 2005;241:1016)
Vomiting
hypokalemia from excess bicarb secretion in kidneys. Gastric outlet obstruction from scarring after chronic ulcer
Dysphagia
difficulty swallowing, pain on swallowing is odynophagia
Oropharyngeal Dysphagia (transfer), almost always organic
Globus hystericus is the feeling that something is caught in the throat
Difficulty with liquids=think neuromuscular
Upper esophageal-webs, carcinoma, zenker’s, left atrial enlargement, aortic aneurysm. Typically progressive as opposed to the intermittent nature of transfer dysphagia
Plummer Vinson
esophageal webs, anemia, spooning of nails, resolves c iron
Dyspepsia
GI cocktail does not work: No benefit to adding donnatal or lidocaine to antacid. Double blind trial (Journal of Emergency Medicine Volume 25, Issue 3 , October 2003, Pages 239-244)
GERD
Caused by reduced pressure in the lower esophageal sphincter, inappropriate transient relaxations of the sphincter, and/or hiatal hernia.
Typical Symptoms: heartburn, regurgitation of food, water brash (hypersalivation)
Supraesophageal/Atypical Symptoms: Chest Pain, Caries, Asthma, Hoarseness, Laryngitis, Cough, Hiccups, N/V
Alarm Symptoms: Dysphagia, Weight Loss, Vomiting, Anemia, GI Bleeding, Early Satiety
The only lifestyle change that has proven effect on GERD is cessation of smoking. Start patients on a once daily PPI. It should be taken 30 minutes prior to eating, as the medication can be destroyed by gastric acid if taken with a meal, but requires food after absorption because only actively secreting pumps are inhibited.
Perforation
Barium bad if perforation, Gastrograffin bad if aspirated
2nd generation cephalosporin and aminoglycoside
SMA syndrome
obstruction of duodenum. After weight loss or bed rest. Crampy PN
Ulcer
pain described as constant and gnawing. Duodenal pain relieved by eating, gastric is exacerbated. Gastric acid output very high at 2 am. Can bleed, perforate, or obstruct
To see free air, must be standing for at least 5 minutes. Can inect 300 cc air through ng to aid visualization. LLR if pt can not stand
Perforation
Left lateral decubitus is actually the most sensitive of the plain film techniques (just as with upright, the patient must stay in position for 10 minutes to achieve maximum sensitivity.)
first get chemical peritonitis
sudden onset peritonitis + free air=perforated viscus
sudden onset + no free air + normal lipase=perforated viscus
graham patch is an omental patch
Upper GI Bleeding
Gastric Volvulus
paraesophageal hernia
Here the gastroesophageal junction lies inside the abdomen but the stomach protrudes through an enlarged paraesophageal defect, unlike hiatal hernia this is a non-sliding hernia.
| | |