Endocarditis
Native: non-viridans strep, strep viridans, enterococci, staph aureus
Prosthetic: coagulase neg. staph (early <60 days postop), Staph Aureus (>60 days post op), Non-viridans strep, enterococci
IVDA/Immunocompromised: staph aureus, strep, gram-negative bacilli
Fever/Anemia/Murmur
Change in mental status due to embolization
Ptechiae, splinter hemorrhages, osler noders (palmar surface of fingertips; tender), janeway lesions (flat macular lesions on the palms; painless), Roths spots (pale c red halo)
Can present with microscopic hematuria (up to 50% of the time)
Get three sets blood cultures from three different sites. Better if separated by time.
Rheumatic Fever
Jones criteria (major)-carditis, polyarthritis, chorea, erythema marginatum (smoke ring of erythema), Sub-Q nodules
Antistrep antibodies stay positive 4-6 weeks post infxn
Native: PCN G and Naf and Genta or Vanco/Genta
Prosthetic: Naf, Genta, Rifampin or Vanco/Genta/Rifampin
virtually all bacteria have been implicated 2. vast majority cause by gram positive organisms a. viridans streptococci most common for abnormal native heart valve IE b. staph aureus most common in injection drug users (normal native valves) and in PV IE c. staph epidermidis (coag staph) relatively common in PV IE 3. fungal organisms in PV IE, immunosuppressed hosts, and indwelling vascular catheters 4. remember the fastidious gram neg bacilli that can cause endocarditis: HACEK organisms that will grow very slowly in culture a. Haemophilus parainfluenza, Haemophilus aphrophilus b. Actinobacillus actinomycetemcomitans c. Cardiobacterium hominum d. Eikenella corrodens e. Kingella kingae
Complications A. embolic phenomenon 1. seen in 22-50% of cases 2. mitral vegetations have highest rate (25%) especially anterior leaflet (37%) – followed by aortic (10%) 3. most cases occur within first two weeks of treatment 4. staph and fungus embolize most frequently 5. CNS most common site (65%) and most of these lodge in MCA 6. Splenic infarct common (40% of left sided IE) but only 5% of these go on to abscess formation 7. ECHO finding risk factor for embolization: vegetations >1 cm in diameter B. periannular infection/abscess 1. very common with prosthetic valve IE (56-100%) 2. 10-40% incidence in native valve IE (AV >MV or TV) 3. AV conduction block may result 4. myocardial fistulae can occur leading to intracardiac shunts 5. prosthetic valve dehiscence leading to CHF 6. rupture into the pericardium also a concern tamponade or purulent pericarditis may result 7. most will need surgery C. acute valvular insufficiency with acute CHF 1. perforation of valve 2. rupture of chordae tendinae 3. dehiscence of prosthetic valve 4. paravalvular leak D. valve obstruction from bulky vegetation 1. fungus is frequent pathogen in this setting 2. less common complication VII. Prophylaxis A. Recommended for whom? 1. High risk a. prosthetic heart valve b. h/o endocarditis c. complex cyanotic CHD (transposition, Tetralogy of Fallot) 2. Moderate risk a. Other congenital heart disease b. Acquired valvular dysfunction (e.g. RHD) c. MVP with regurgitation (or thickened leaflets) d. Hypertrophic cardiomyopathy 3. Not recommended a. isolated secundum ASD b. Surgical repair of ASD, VSD, or PDA c. MVP without regurgitation d. Previous CABG e. functional or physiologic heart murmurs f. pacemakers and implanted defibrillators B. For which ED procedures? 1. dental procedure causing gingival bleeding 2. insertion of FC when UTI is present – controversial 3. I&D of abscess 4. Bronchoscopy C. Which antibiotics: 1. Oral or respiratory procedures b. amoxacillin 2 g po one hr pre-procedure (15 mg/kg for children) c. NPO: ampicillin 2 g IV or IM within 30 pre-procedure d. PCN allergic: clindamycin 600 mg, or cephalexin 2 g, clarithromycin/azithromycin 500 mg po 1 hr pre-procedure e. NPO/PCN allergy: clindamycin 600 mg IV or cephazolin 1 g IV/IM within 30 pre-procedure 2. GU procedures a. high risk: ampicillin 2 g and gentamicin 1.5 mg/kg IV/IM within 30 of procedure; 6 hr later, ampicilling 1 g iv/im or amoxacillin 1 g po; substitue single dose of vanco if PCN allergy b. moderate risk: amoxacillin 2 g po one hr pre-procedure or ampicillin 2 g IV/IM within 30 of procedure 3. Skin/soft tissue abscess (non-oral) a. dicloxacillin or cephalexin single dose one hr pre procedure b. vancomycin for those NPO or PCN- allergic SELECTED REFERENCES 1. Wilson WR, Karchner AW, Dajani AS, et al: Antibiotic treatment of adults with infective endocarditis due to steptococci, enterococci, staphylococci, and HACEK microorganisms: American Heart Association. JAMA 1995;274:1706. 2. Bayer AS, Bolger AF, Taubert KA, et al: Diagnosis and management of infective endocarditis. Circulation 1998;98:2936. 3. Dajani AS, Taubert KA, Wilson W, et al: Prevention of bacterial endocarditis: recommendations by the American Heart Association. JAMA 1997;277:1794. 4. Bayer AS: Infective endocarditis. Clin Infect Dis 1993;17:313. 5. Anonymous. Management of infective endocarditis. Drug & Therapeutics Bulletin. Apr. 2002 404):26-30. 6. Barnes PD, Crook DW. Culture negative endocarditis. Journal of Infection. 1997; 35(3):209-13. 7. Delahaye F, Hoen B, McFadden E, et al. Treatment and Prevention of infective endocarditis. Expert Opinion on Pharmacotherapy. 2002; 3(2):131-45 8. Giessel BE, Koenig CJ, Blake RL Jr. Management of bacterial endocarditis. American Family Physician. Mar 2000 61(6):1725-32. 9. Hoesley CJ, Cobbs CG. Endocarditis at the millennium. Journal of Infectious Diseases. Mar. 1999 179 Suppl 2:S360-5. 10. Keys TF. Infective endocarditis: prevention, diagnosis, treatment, referral. Cleveland Clinic Journal of Medicine. May 2000 67(5):353-60. 11. Mauri L, de Lemos JA, OGara PT. Infective Endocarditis. Current Problems in Cardiology, Sep. 2001 26(9):562-610.Farmer JA, TorreG. Endocarditis. Current Opinion in Cardiology. Mar 1997 12(2:123-30 12. Pawsat DE, Lee JY. Inflammatory disorders of the heart. Pericarditis, myocarditis, and endocarditis. Emergency Medicine Clinics of North America. Aug. 1998 16(3):665- 81. 13. Piper C, Korfer R, Horstkotte D. Prosthetic valve endocarditis. Heart (British Cardiac Society) May 2001 85(5):590-3. 14. Stamboulian D, Carbone E. Recognition, management and prophylaxis of endocarditis. Drugs Nov. 1997 54(5):730-44.
Prophylaxis
(1) a prosthetic valve of any kind, (2) a history of prior IE, or (3) a history of congenital cyanotic heart disease
EASE trial just reported shows early surgery should be the path instead of intial medical management
Valvular Heart Disease
Prosthetic Valves
Mechanical
Last ~20 yrs, SEM murmur
Bioprosthetics
human, porcine, or bovine
8-10 yrs
anticoagulation optional, usually aspirin
Both types are prone to thromboembolism.
Valves may fail leading to acute regurgitation
Paravalvular leak from disruption from annulus, can result from endocarditis
Endocarditis
Hemolysis
Get CBC, LDH, PT/PTT, ESR, Blood CX,
Aortic valves are lower risk for clot than mitral
The peak incidence of thromboembolism is during the first 3 months after surgery, probably reflecting the lack of endothelialization of the newly implanted prosthetic materials and delay in achieving therapeutic anticoagulation in the early days after operation
Mitral Valve Prolapse
can be associated with chest pain, palpitations, and hyperventilation in females.
May need b-blockers, dental prophylaxis,
Mitral Stenosis
from rheumatic heart disease, congenital, or left atrial myxomas
exertional dyspnea, hemoptysis, CHF sx
Can lead to a-fib, embolization
Mitral Regurgitation
acute is from ruptured chordae or papillary muscle dysfunction
chronic is most commonly from rheumatic or MVP, also Marfan’s
rate control, diuretics, anticoagulate
These patients need afterload reduction
Aortic Stenosis
congenital bicuspid valve, rheumatic heart disease, calcific aortic stenosis.
DOE, angina, exertional syncope, CHF, sudden death
Harsh systolic murmur
Symptomatic patients are at risk for sudden death, refer for valve surgery.
Most common cause in ICUs is senile calcific disease Causes LVH which predisposes to subendocardial ischemia
tachycardia decreases diastolic filling and therefore decreases coronary blood flow
Pts present with exertional dyspnea, angina, syncope, may progress to heart failure
Diuresis, IVF, and venodilators can all cause deterioration
avoid hypotension
Unload trial would say nitroprusside is a good move
OVERVIEW
Obstruction can be
- supravalvular
- valvular (most common)
- subvalvular
SEVERITY ASSESSMENT
- appearance
- mobility
- gradient
— continuous wave Doppler allows peak velocity to be measured -> peak gradient can be calculated using Bernoulli equation
— peak gradient = 4 x peak velocity across the narrowing squared
— normal peak gradient < 10mmHg, critical > 70mmHg
— gradient measurements are very dependent on ventricular function so can be misleading. - area
— normal 2.5-5.5 cm2
— critical < 0.92 cm2 - dimensionless severity index = ratio of LVOT velocity/aortic valve velocity (V1/V2)
— provides a dimensionless measurement of aortic stenosis which is independent of Q
— < 0.25 implies a valve area of 0.75cm2 (severe AS) - complications:
— LV hypertrophy or dilation
— LV systolic and diastolic dysfunction
— post-stenotic dilation
CATEGORIES OF AORTIC STENOSIS SEVERITY (From Vahanian et al, 2010)
| Aortic sclerosis |
Mild | Moderate | Severe | |
|---|---|---|---|---|
| Aortic jet velocity (m/s) | <2.6 | 2.6–3.0 | 3–4 | >4 |
| Mean gradient (mmHg) | — | <30 (25) | 30–50 (25–40) | >50 (40) |
| AVA (cm2) | — | >1.5 | 1.0–1.5 | <1.0 |
| Indexed AVA (cm2/m2) | >0.9 | 0.6–0.9 | <0.6 | |
| Velocity ratio | >0.50 | 0.25–0.50 | <0.25 |
Above from Life in the Fast Lane CCC
Aortic Insufficiency
acutely from infective endocarditis, dissection, trauma
chronic from rheumatic heart disease, bicuspid valve, marfan’s
widened pulse pressure
try judicious use of nitro or nitroprusside
reduce bradycardia to decrease diastolic filling and therefore degree of regurg
never use IABP
Withholding Anticoagulation
much more dangerous in mitral and tricuspid
can hold aorta anti-coag 2 days before surg and drift INR t to <=1.5
then restart
for mitral/tricusp bridge with heparin until procedure
(Emerg Med Clin 2011;29:801)
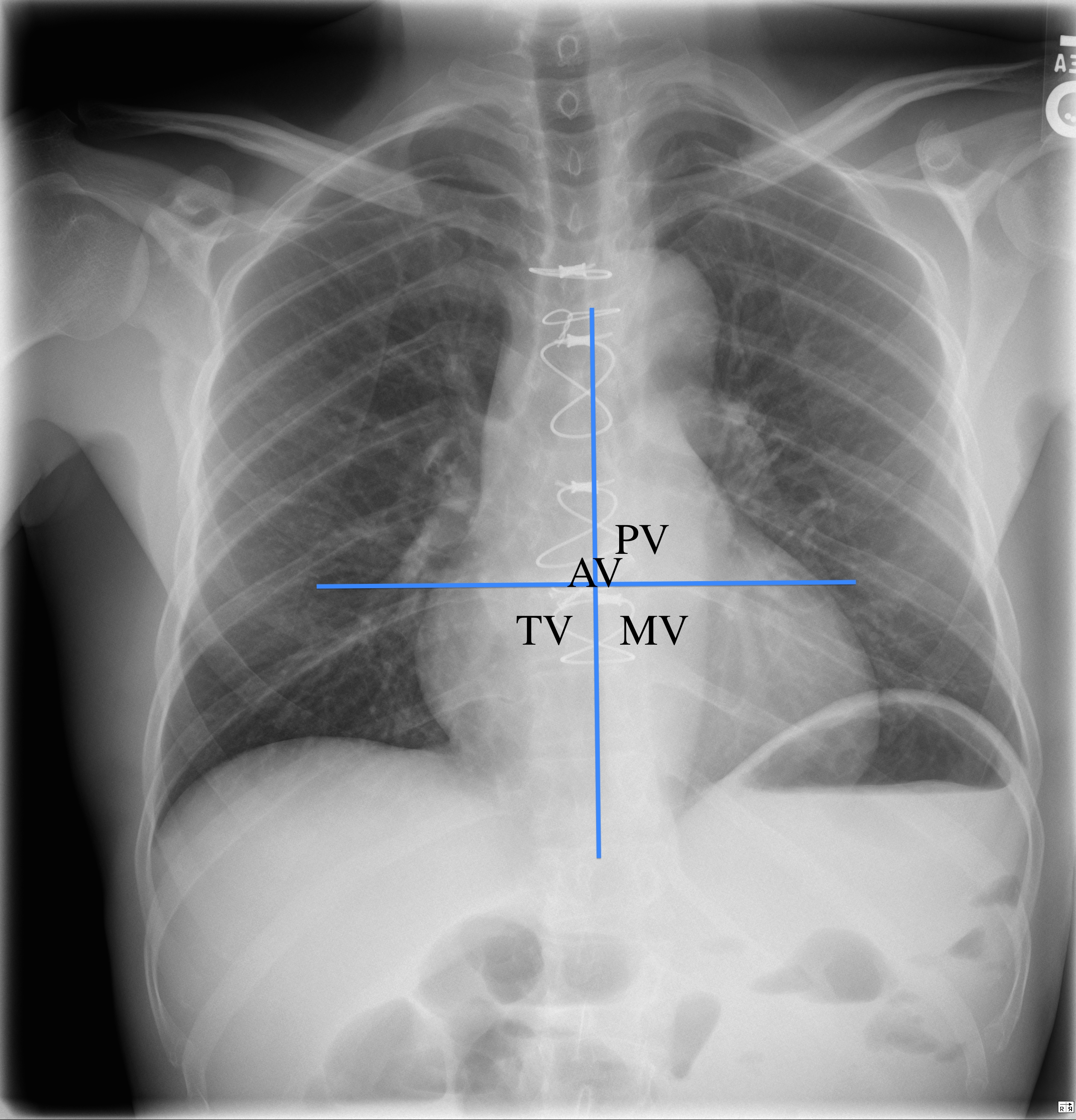
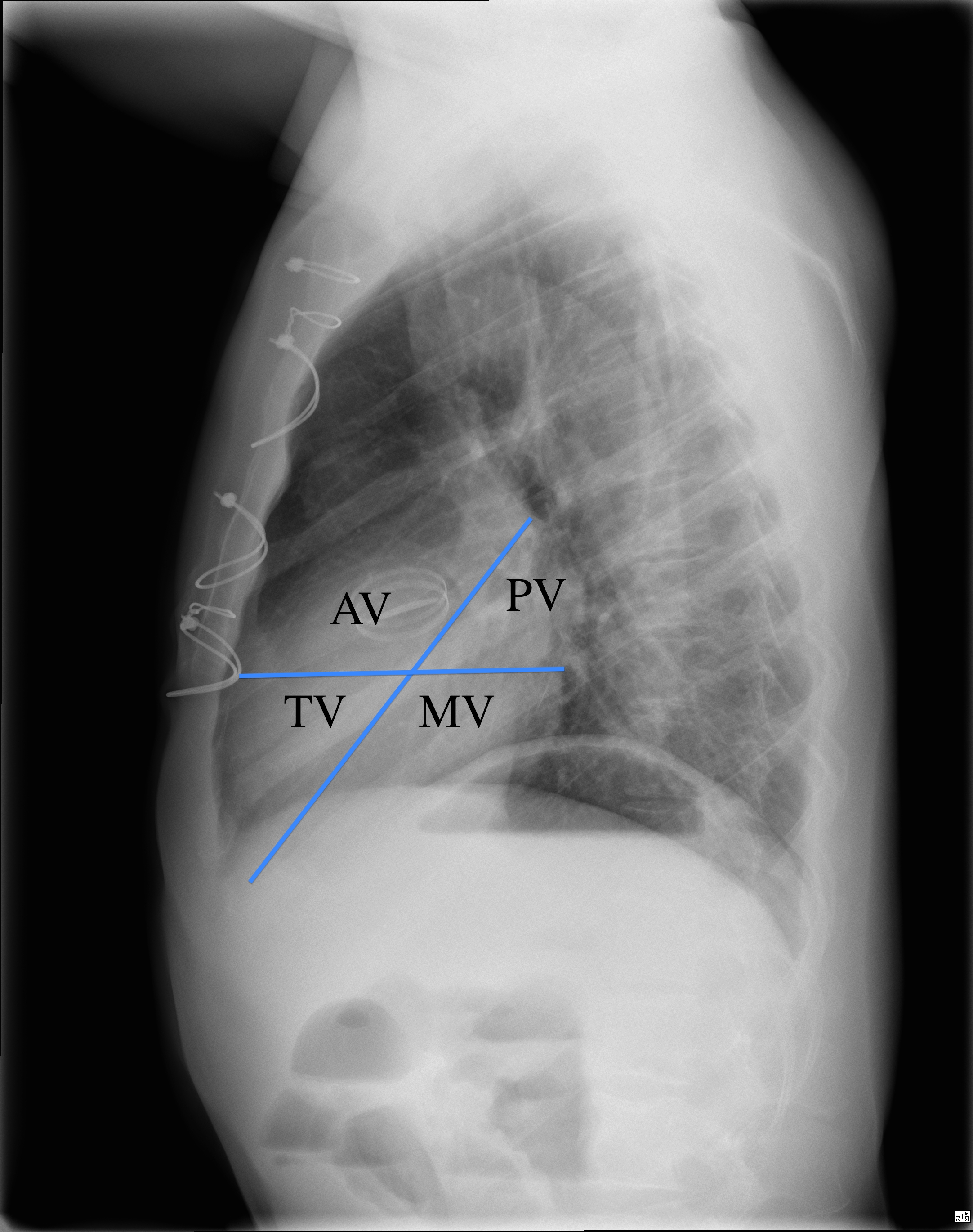
Which Valve has been Replaced?
http://www.raddaily.com/whitepaperarticle.php?articleTitle=Cardiac+Valves:+Assessment+and+Identification