Acute Arthritis
Septic Arthritis
Evidence basis for dx of Septic Arthritis (Acad Emerg Med. 2011;18(8), 781-96)
Monoarticular
Consider trauma, lyme, STDs, IVDA, gout
Joint Aspiration (In order)-CX, Gram Stain, Glucose (Must be fasting 6 hrs), WBC, Lactate
Serum CBC and ESR
Rx-Drainage (medical or surgical), and Abx. Hips and Prostheses need surgical. Gonorrhea just ABX.
For knee arthrocentesis, try using an 18 gauge spinal needle: It has a great obturator to prevent skin biopsy, allows easy manipulation in the joint, and changing syringes is a snap! (Henry J. Siegelson, MD, FACEP) Editor’s note: also, if there is significant blood in the effusion, you can prevent clotting (to get an accurate red cell and white cell count) by putting about 1/10 to 1/4 cc of Heparin solution in the syringe before aspirating the knee. (Alan Clark)
Generally, for routine analysis, the SF sample is sent for WBC count and differential, crystals, Gram stain, and culture. In certain cases, when patients are chronically ill or immunocompromised, fungal and mycobacterial cultures may be indicated. Because inflammatory fluid can clot, it should be anticoagulated (5). If adequate sample is obtained, SF for cell count should be collected in a lavender-topped tube containing liquid ethylenediaminetetraacetic acid (EDTA) anticoagulant. The culture tube or syringe must remain sterile (6). Synovial fluid to be analyzed for crystals may also be collected in a lavender-topped tube containing liquid EDTA, but it is generally recommended by most authors that a green-topped tube containing sodium heparin be used for crystal analysis (7). Glucose and other chemistries do not require anticoagulant and may be sent in a red-topped tube.
Although volume requirements vary among laboratoriess, approximately 1 mL of fluid is required for an accurate cell count and generally 23 mL of SF is adequate to run all appropriate tests. If only a few drops are obtained, the sample should be sent for crystals and culture, which are most diagnostic (12). One study suggests that leukocyte counts for non-inflammatory SF can be grossly estimated on wet drop preparations using only one to two drops of fluid. Clayburne et al. showed that the observation of 0 to 2 WBC per high power field (HPF) while examining 10 HPF could accurately predict a leukocyte count less than 1300/mm3 (13). To avoid misdiagnosing borderline inflammatory fluids, it is very important for SF to be analyzed soon after it is obtained because cell counts and examination for crystals lose accuracy within hours. Kerolus et al. reported that the SF WBC and % PMNs can decrease within only a few hours after aspiration and crystals were less abundant and more difficult to recognize by the next day. This rate of disintegration was dependent on the time elapsed after aspiration and was more rapid in fluids kept at room temperature than in those refrigerated (14).
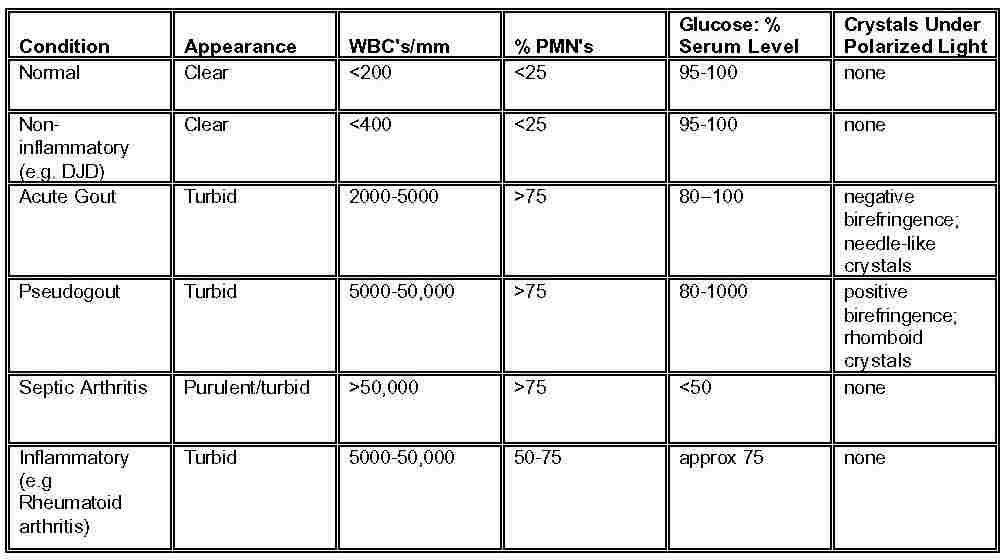
A major difference in serum and SF glucose may add support to the diagnosis of infectious arthritis, especially if the initial Gram stain is negative. The normal glucose level in SF is usually within 1020 mg/dL of the fasting serum glucose level (31). A SF glucose level > 50 mg/dL less than that in simultaneously drawn fasting serum (6 h post-prandially) strongly suggests an infectious process (2). SF glucose metabolism via the anaerobic pathway occurs in several conditions, but most commonly in infection (21). However, SF glucose as well as protein are highly inaccurate markers of inflammation and are generally less informative than other studies. For this reason, the ordering of chemistry studies for SF should be discouraged because they are likely to provide misleading or redundant information (19). In addition, obtaining a > 6 h post-prandial blood sample to allow for the equilibrium of serum and synovial glucose is in most cases impractical in the ED environment. In one study, the SF glucose result accurately categorized the arthropathy as inflammatory or non-inflammatory in < 50% of cases (19). Another studied showed the sensitivity of the SF glucose for detecting inflammatory joint disease was only 20% and specificity was 84%, using a cutoff of 75 mg/dL among those patients studied (18). Therefore, the general insensitivity and non-specificity of SF glucose would argue against including the SF glucose as a routine part of SF analysis. Nonetheless, there may be certain clinical situations in which obtaining a SF glucose is useful. For example, in the case of a patient presenting with an inflammatory monoarthritis and prior antibiotic therapy, a significantly reduced SF glucose may raise suspicion of septic arthritis in the situation where the Gram stain and culture are falsely negative (18).
SYNOVIAL FLUID ANALYSIS

Articular vs. periarticular (no pain c passive motion)
Pseudogout positive, gout negative
Septic is usually considered >50,000 WBC in joint fluid, however, septic arthritis can certainly exist at lower levels. Sensitivities for WBC,ESR, or jWBC in adults who had septic arthritis were 48%, 96%, and 64% respectively. If all three are normal, then perhaps you can rule out septic arthritis. (Academic Emergency Medicine Volume 11, Number 3 276-280)
Monoarticular
Gout
Rx c colchicine (.6 mg PO q 1 h until relief, max 10 doses) or NSAIDS
thiazides predispose
Does this pt have septic arthritis? JAMA 2007;297:1478 Negative ESR (0.17) LR of synovial WBC<25000 (0.32) >25000 (2.9) >50000 (7.7) >100000 (28) >90 poly (3.4) <90 (0.34) LDH<250 (0.1)
ESR>25 for septic arthritis, fairly sensitive but not specific
Polyarthritis
Gonococcal-full orifice culture, assoc c synovetendinitis
Viral-rubella and Hep B
Seronegative spondyloarthropathies
Ankylosing spondylitis-bamboo spine
Reiter’s, Psoriatic,
Rheumatic fever-
Jones (2 major)-carditis, polyarthritis, chorea, erythema marginatum, sub-q
Medications
Celebrex touts their decreased numbers of ulcers as a reason to use the drug, but the Class study showed decreased ulcers with celebrex during the first half of the studies and then an increased risk in the second half. Only the first half of this two part study was reported. (Br Med J 324:7349, 2002)
Gout (Emedhome.com)
Acute Gouty Arthritis in the ED
Emergency Physicians frequently evaluate patients with attacks of acute gouty arthritis (“gout flare”) that characteristically present as an attack of synovitis, which can be severe. Recent guidelines and expert opinion address issues that often come up with such ED patients:
1. For attacks of mild/moderate gout severity involving one or a few small joints or 1-2 large joints*, monotherapy is appropriate. Options are:
- NSAIDs – full dose (if appropriate) until the attack completely resolves.
- Corticosteroids – Prednisone 0.5 mg/kg/d for 5-10 days OR 2-5 days then taper for 7-10 days. Methylprednisolone dose pack is an alternative. Consider intra-articular corticosteroids if the attack involves 1-2 large joints.
- Colchicine – only for attacks of onset < 36 hours prior to presentation. If the patient is already on colchicine and has received acute gout regimen colchicine within the last 14 days, select another monotherapy. Give 2 tablets (1.2 mg) followed in one hour by a third tablet (0.6 mg), followed by 0.6 mg once or twice daily (unless dose adjustment is needed) 12 hours later, until the attack resolves.
*large joints = ankle, knee, wrist, elbow, hip, or shoulder
2. For acute attacks with severe pain, particularly a polyarticular attack or an attack affecting multiple large joints – use combination therapy of colchicine and NSAIDs, oral corticosteroids and colchicine, or intra-articular steroids with any of the other modalities.
3. If a patient returns to the ED with an acute attack not responding adequately to initial monotherapy, then switch to another monotherapy or add a second agent (inadequate response has been defined as either, < 20% improvement in pain score within 24 hours, or < 50% improvement in pain score > 24 hours).
4. Do not stop the patient’s urate lowering therapy during an acute attack – symptoms would only worsen if it is stopped or adjusted during the flare.
5. During the initial phase of urate lowering therapy, there is actually an increase in acute gout attacks. Patients should be reassured that this is expected and they should not discontinue their new medications.
References:
(1) Khanna D, et al. Arthritis Care Res 2012 Oct;64(10):1447-61.
(2) Harrold L. Curr Opin Rheumatol 2013 May;25(3):304-9.
Acute Gouty ArthritisThis case of acute gouty arthritis of the 1st metatarsophalyngeal joint provides an opportunity to highlight several important concepts: Acute gout may occur in the presence of normouricemia: It has been well established that acute gouty arthritis not uncommonly occurs in the setting of normal serum uric acid levels. In fact, one author has suggested that serum uric acid determinations are of little value in the assessment of possible gout, and that gout and hyperuricemia should be regarded as separate phenomena (1). Clearly, the physician attending to this patient during the first visit was fooled by the lack of an elevated serum uric acid, and the presence of a low grade fever and an elevated WBC, both of which may accompany acute gout. Consider treatment with steroids if the risk of side effects from NSAID’s is judged to be too high: Nonsteroidal anti-inflammatory drugs, which are currentlyfavored for the treatment of acute gouty arthritis, are rapidly effective but may have serious side effects. This patient exhibited several contraindications to NSAID use (peptic ulcer disease, renal insufficiency). Corticosteroids, administered either intraarticularly or parenterally,are used increasingly in patients with monarticular gout (1). Intraarticular injections of a corticosteroid are usually veryeffective in patients with acute monarticular gout, and their use is becoming more widespread as experience with the diagnostic aspiration of joints increases (2). Indeed, aspirationalone can sometimes greatly reduce the pain of gout. The appropriatedose of corticosteroids is related to the size of the joint;an intraarticular dose of methylprednisolone acetate rangesfrom 5 to 10 mg for a small joint to 20 to 60 mg for a largejoint such as the knee. Systemic corticosteroid therapy is another option when NSAID’s are contraindicated. There are reports ofgood responses, without a rebound effect, to oral prednisone(30 to 50 mg per day initially, with the dose tapered duringa period of 7 to 10 days), intramuscular corticotropin (40 U)or triamcinolone acetonide (60 mg), or intravenous methylprednisolone(a daily dose of 50 to 150 mg administered during a 30-minuteperiod, with the dose tapered during a period of 5 days) (1,2). Colchicine is less favored now than in the past,because its onset of action is slow and it invariably causesdiarrhea. Furthermore, colchicine is less effective once an acute attack has persisted for a few days (2).Therapy thatmight alter serum urate concentrations should not be initiatedor changed in the ED as long as any gouty joint inflammation persists: Two classes of drugs are available to correct hyperuricemia: uricosuric drugs and xanthineoxidase inhibitors. A potential complication of these drugs is the precipitationof acute attacks of gout. The mechanism is poorly understood,but it is usually attributed to the sudden change in the serumurate concentration (1). The risk can be minimized by delaying urate-lowering therapyuntil several weeks after the last attack of gout. It is important to make an accurate diagnosis of gout before beginning therapeutic intervention (2): This is especially true in a patient such as the one on the previous page who has never before been diagnosed with gout. A definitive diagnosis requires aspiration and examination of synovial fluid to confirm the presence of monosodium urate crystals. Even the smallest amount of fluid obtained from the shaft or hub of the needle during aspiration can be examined for crystals. Monosodium urate crystals are identified by examination under polarized light microscopy. Confirmation of the presence of monosodium urate crystals is imperative so that patients, for example, with coincidental hyperuricemia and osteoarthritis are not incorrectly diagnosed with gout and unnecessarily treated with medications such as allopurinol. Furthermore, rheumatoid arthritis, calcium pyrophosphate dihydrate deposition (pseudogout), spondyloarthropathies and osteoarthritis may also mimic gouty arthritis.
Podagra is inflammation of the first MTP joint.
Osteoarthritis
No sig. benefit in pain scale to bextra or naproxen, only slightly less ulcer complications with bextra (J Fam Pract 51(6):530, June 2002)
Arthrocentesis
Put 5 mg of morphine in 5 cc of Bupivicaine and 15 cc of NS and inject into the knee space.
| | |