Best Review Article from STC folks ( J Crit Care 2013;28:1019)
Optimal Dosing (Crit Care 2011;15:207) 20-35 ml/kg/hr seems optimal replacement fluid rate
Optimal Effluent Rate 25mL/kg/hr
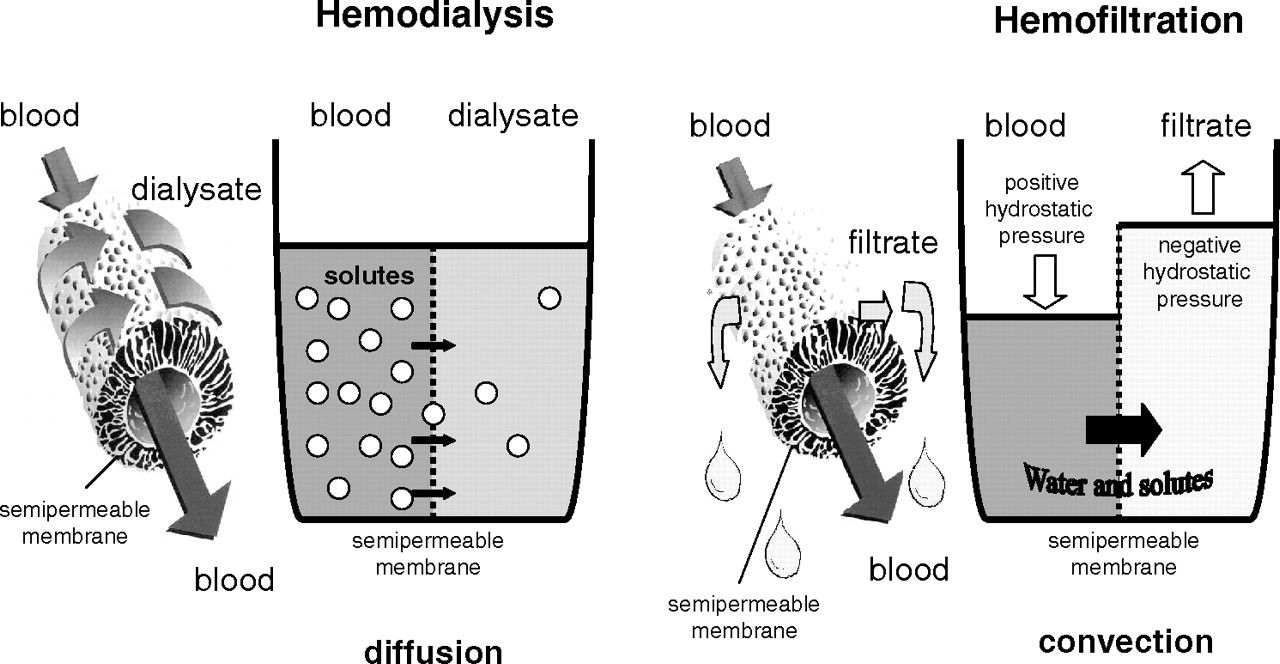
Dialysis is from the Greek for to pass across.
Ultrafiltration and Dialysis are the two sides of the RRT picture
Dialysis: diffusion of small particles across a semi-permeable membrane along a concentration gradient. Solute transport is proportional to flow rate.
Ultrafiltration: carries small and middle sized particles across a semi-permeable membrane when dissolved in solution by a process known as solvent drag. Also proportional to flow rate.
Intermittent HD is the quickest allowing large fluid offloading, but many patients become hypotensive. Since crit ill patients are already usually intravascularly depleted, the further insult from post-HD hypotension can cause ischemic damage to many organs including the already damaged kidneys.
70% Pre and 30% Post
20-25 ml/kg/hr
Hypernatremia, met alkalosis are complications of trisodium Citrate
Indications A-E-I-O-U
Acidosis
Electrolyte Abnormalities
Intoxication
Overload of Fluids
Uremia (Pericaditis, Mental Status Changes)
Modern Criteria for the Initiation of Renal Replacement Therapy (RRT) in the Intensive Care Unit[*]
Oliguria (urine output < 200 mL/12 hours)
Blood urea nitrogen > 80 mg/dL
Serum creatinine > 3 mg/L
Serum potassium > 6.5 mmol/L or rapidly rising
Pulmonary edema unresponsive to diuretics
Uncompensated metabolic acidosis (pH < 7.1)
Temperature > 40° C
Uremic complications (encephalopathy/myopathy/neuropathy/pericarditis)
Overdose with a dialyzable toxin (e.g., lithium)
*
If one criterion is present, RRT should be considered. If two criteria are simultaneously present, RRT is strongly recommended.
Small Solutes
(<300D)
Middle Molecules
(500-50000D)
Low Molecular Weight Proteins
(5000-50000D)
Large Proteins
(>50000D)
Urea, Creatinine, Amino Acids Myoglobin,B12, Vancomycin Inflammatory Mediators Albumin
1M=1 g atomic weight of solute in 1 liter of solution
1N=for single charge same as above, for doubly charged such as Ca, 1N=0.5M
substance that forms ionized particles is an electrolyte
convective transport is solvent drag
sieving coeeficient amount of solute convected across a membrane in proportion to quantity of fluid
CVVH relies on transmembrane pressure negative on one side or positive on the other
Dialysis Membrane
Two types:
Cellulose-aka low flux membranes, can activate inflammatory mediators including complement cascade. This can make them dangerous in ICU patients.
Synthetic-no reactivity. Also properties make ultrafiltration “built-in” even if not specifically hooked up for this mode. The standard for critically ill patients.
Dialysis Disequilibrium Syndrome syndrome of dizziness, nausea, possibly seizures after dialysis. Usually when a uremic patient has first HD; presumed to be caused by rapid flow of water into brain cells which have become relatively hyperosmolar.
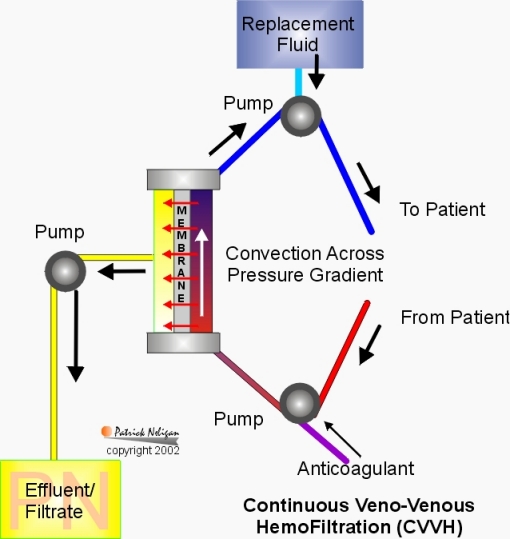
CVVH
Continuous Venous Venous Hemofiltration filters middle sized particles and can take off up to 1 liter per hour
Need replacement fluids
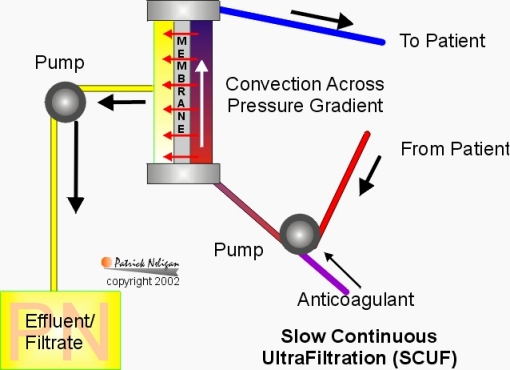
SCUF Slow continuous ultrafiltration, ideal for removing fluid overload, can remove 300-500 cc/hr
No replacement fluids needed
CVVHD
Continuous Venous Venous Hemodialysis
Small particle filtration and fluid removal
Need dialysate
CVVHDF
Continuous Venous Venous Hemodiafiltration
Combination of both of the above modes, filters small and medium particles
Need fluid replacement and dialysate

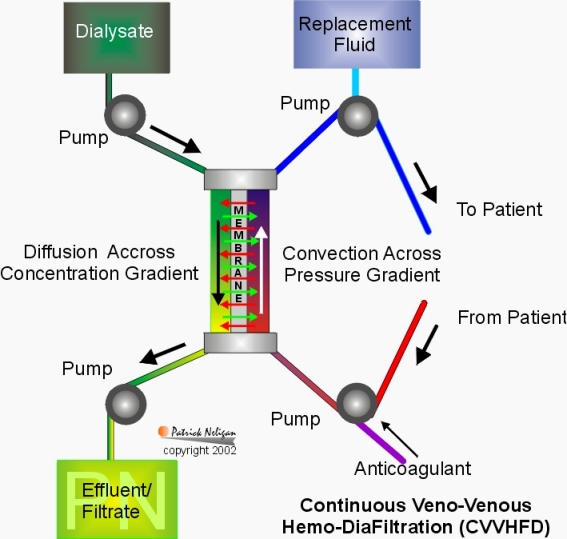
CVVHDF is similar to IHD in slow motion: the blood flow is 100 200ml/min (usually set at 120), the dialysate flow is 1000ml/hour, the filtration rate is 10-20ml/hour (very efficient), the urea clearance is 10-20ml/hour.
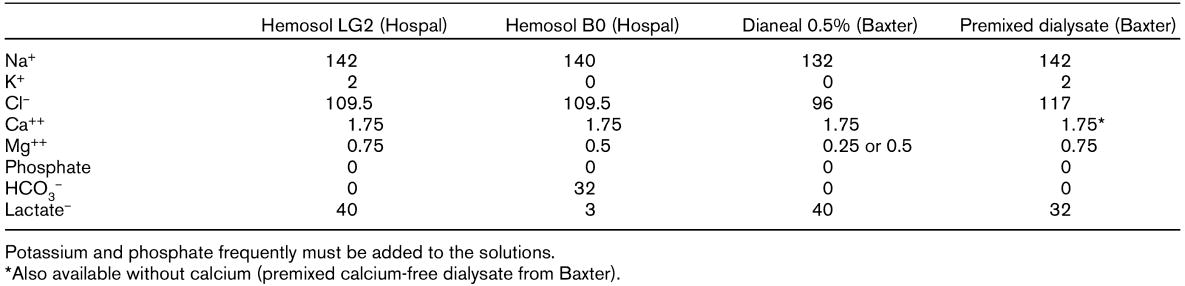
Usually, you will use Lactated Ringers solution as dialysate and replacement as this is the easiest to obtain fluid that closely matches physiologic. Over time, the blood will tend towards the dialysate.
KPO4 supplementation is often necessary. Note also that there is no NaHCO3 in the dialysate, leading to loss of bicarbonate: compensated for by the passage of lactate (anionic, a base) into the bloodstream. Calcium may also be required, although Ca and HCO3 cannot be given together, because they precipitate. This is usually metabolized into bicarbonate in the liver. In liver failure, it is wiser to use a lactate free dialysate such as normal saline, add give bicarbonate supplementation. (Neligan, Patrick)
Anticoagulation is also necessary. Since heparin has a number of disadvantages, other agents are often used.
Xigris will cover RRT anticoagulation
RRT has a role in sepsis as well, as inflammatory mediators can be eliminated from the blood stream
Bacteria can be recovered from the ultrafiltrate in CRRT (Crit Care Med 2004 32, p.932)
Patients will not spike a temp on CRRT
Settings
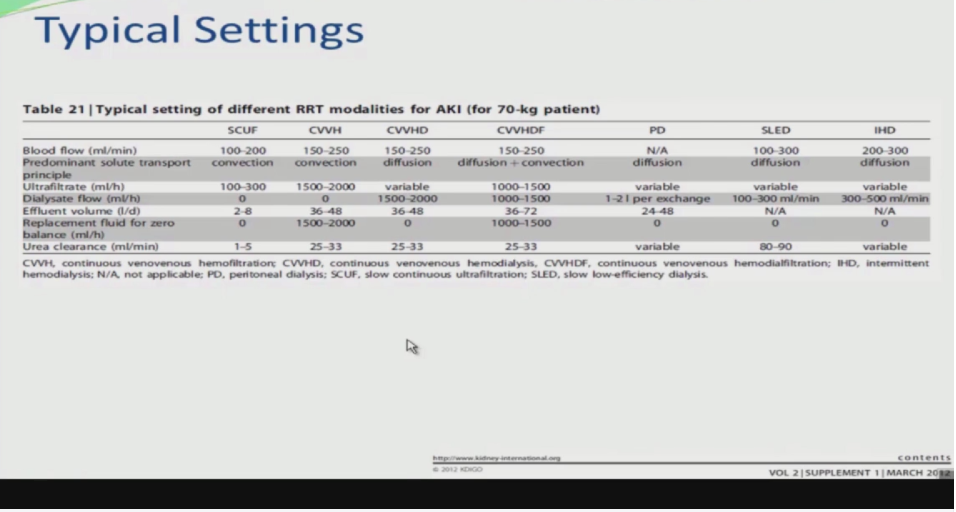
Shoot for 25 ml/kg/hr
CVVH
Pick Replacement Fluid
Set UF rate
Set Qb (Blood Flow) Usually 200 cc/min (Perhaps max should be 150, above this level machine may read more flow, but probably resistance limited)
Set Effluent Rate 2-3 L per hour
CVVHD
Set UF Rate
Set Blood flow 80-200 cc/min (120)
Dialysis Flow 2-3 L/hour
Dialysate Plasmalyte or 1/2 NS with 1 1/2 Amps Bicarb
D 1.5 1/2NS with one amp bicarb, 6cc 23.4% NaCl, 1.5 mEq/L MgSO4 and 0-4 mEq/L of K
Tri-sodium citrate at 15 mmol/hour
CaCl drip 4 grams in 500 cc NS, run @200 mg/hour
Titrate to maintain ionized Ca 1.15-1.29
or
Heparin bolus 40 U/kg then 10 U/kg/hour
I think that before speaking about a “vogue” for HV-CRRT, we have to stick on facts.After the PRT of Ronco (425 patient/Lancet 2000) assessing the adequate dose of CRRT during ICU-ARF(Mainly Non Septic).The best dose in terms of survival was 35 ml/kg/h of HF.So, normally we should apply this dose for every ICU-ARF and this might not be so easy with some machines as for larger patients, you may need blood flow around 300 ml/min to keep the filtration fraction below 25 %.
Bad humour filtration; need PAN filter and >50 L/day
Dose associated with decreased mortality 35 cc/kg/hour (Lancet 2000;356:26)
Weaning
Leave Qb as it is
When BUN gets to between 30-40, start weaning Qd
Can do creatinine clearance using urinary creatinine.
Elahi, MN, et al. Early hemofiltration improves survival in post-cardiotomy patients with acute renal failure. Eur J Cardiothorac Surg. 2004 Nov;26(5):1027-31. Warnholtz A, Slater AD, Golper TA. Continuous arteriovenous hemofiltration in the critically ill patient. Anesthesiology. 2004 Aug;101(2):327-39. Stein B, Pfenninger E, Grunert A, Schmitz JE, Deller A, Kocher F. The consequences of continuous haemofiltration on lung mechanics and extravascular lung water in a porcine endotoxic shock model. Intensive Care Med. 1991;17(5):293-8. Resuscitation. 1986 Jan;13(2):123-32. Hemofiltration in septic ARDS. The artificial kidney as an artificial endocrine lung.Gotloib L, Barzilay E, Shustak A, Wais Z, Jaichenko J, Lev A. Twenty-four patients with high microvascular permeability pulmonary edema were initially treated by means of conventional supportive therapy for 1-12 days. Continued deterioration was treated by predilutional hemofiltration and induced a dramatic improvement in 22/24 patients. Survival was 92%. Sieving coefficients for autacoids and middle molecular weight vasoactive peptides involved in the development of high microvascular permeability pulmonary edema were higher than 0.88 indicating that clearing from blood of these peptides during one pass through the hemofilter is similar to that obtained during one pass through the pulmonary normal microvasculature. Hemofiltration seems to be a significant breakthrough in the treatment of ARDS secondary to severe sepsis. Anesthesiology. 2004 Aug;101(2):327-39. Hemofiltration but not steroids results in earlier tracheal extubation following cardiopulmonary bypass: a prospective, randomized double-blind trial.Oliver WC Jr, Nuttall GA, Orszulak TA, Bamlet WR, Abel MD, Ereth MH, Schaff HV. Mayo Medical School, Rochester, Minnesota, USA. oliver.william@mayo.edu BACKGROUND: Activation of the inflammatory cascade is thought to account for some of the respiratory dysfunction and prolonged mechanical ventilation associated with cardiopulmonary bypass. The objective of this investigation was to identify whether perioperative steroids or hemofiltration during cardiopulmonary bypass, by their attenuation of inflammation, would reduce duration of mechanical ventilation after cardiac surgery. METHODS: After Institutional Review Board approval and informed consent, 192 patients scheduled to undergo elective primary coronary artery bypass grafting or valvular replacement or repair were randomized in a double-blind prospective study into three groups. One group (Control) received saline at induction and at 6-h intervals for four doses. Another group (Hemofil) received saline and hemofiltration to obtain 27 ml/kg of hemofiltrate. The final group (Steroid) received 1 g methylprednisolone before anesthesia induction and then 4 mg of dexamethasone at 6-h intervals for four doses. All patients underwent normothermic cardiopulmonary bypass and received propofol for postoperative sedation. Separate two-sample comparisons were performed to compare each experimental group versus the control group using the Wilcoxon rank sum test for continuous variables and Fisher exact test for categorical variables. In all cases, two-tailed P values </= 0.05 were considered statistically significant. RESULTS: The median time until the patient reached an intermittent mandatory ventilation of 4/min (258.5 versus 385.0 min, respectively; P = 0.02) and tracheal extubation (352.0 versus 518.0 min; P = 0.03) was significantly reduced for group Hemofil but no different for Steroid compared to Control. CONCLUSIONS: Hemofiltration and steroids are both previously reported to attenuate the inflammatory response but only hemofiltration reduced time to tracheal extubation for adults after cardiopulmonary bypass in this study.
SH 44 HEP “bufferfree” dialysate for citrate CVVH, 5L bags, containing: Na+ 109,5 mmol/L K+ 2,08 mmol/L Ca++ 1,81 mmol/L Mg++ 0,52 mmol/L Cl- 116,24 mmol/L Lactate- 3,00 mmol/L Glucose 5,80 mmol/L (1,04g) We also use their standard bicarbonate buffered dialysate, SH 53 HEP, 5 L, containing two compartments, 0,5 L acids and 4,5 L base and when mixed: Na+ 140 mmol/L K+ 2,0 mmol/L Ca++ 1,25 mmol/L Mg++ 1.0 mmol/L Cl- 108,5 mmol/L Lactate- 3,00 mmol/L HCO3- 35,0 mmol/L Glucose 1,0 g/L Use of dialysate is per protocol, and depends mainly on bicarbonate of arterial blood of the patient. We frequently need to give supplementary Ca++ iv, as this may decrease through binding with the citrate. We use a housemade trisodiumcitrate solution of 500mmol/L (15%) with a pH of 6. Machine: Multifiltrate made by Fresenius Filter: Nipro UF-205; 1,9 square meter We run the CVVH in post-dilution mode only; with bloodflow of 200 ml/min and substitution of 3000 ml/h. Citrate runs on 70 ml/h We check Na, K, Cl, Ca (ionised) and bloodgas every 6h and adjust according to results: HCO3 < 21; aniongap <15: lower the amount of bufferfree dialysate, give more bicarbonate buffered dialysate. HCO3 < 21; aniongap >15, Ca<0,8: cumulation of citrate: lower citrate of increase substitutionflow HCO3 < 21; aniongap >15, Ca>0,8: use less bufferfree substitution (or there is lactate accumulation) HCO3 21-25, Ca>0,8: this what we want HCO3 21-25, Ca<0,8: extra Ca++ iv HCO3 >25: too much buffer, use more bufferfree dialysate
Sieving coefficient of hemofilters for Na, Cl, HCO3 are 1

Acetate is processed by liver and muscle to bicarb 1:1
citrate is 1:3
lactate is 1:1
Making Solutions:
To 1 liter of 1/2 NS add: 4 meq KCL 29 meq NaCl 44 meq NaAcetate
250 mg of MgSO4 to yield Na 150 K 4
Mg 2 Cl 110 Acetate 44 for reference Plyte A is: Na 140 K 4 Mg 3 Cl 98 Acetate 27 Gluconate 23 each 100 cc of plyte a contains 526 mg NaCl 502 mg NaGluconate 368 mg NaAcetate 37 mg KCl 30 mg MgCl pH adjusted to 7.4 with NaHydroxide Osm 294
Note:
1 Gram of MgSO4 contains 8.1 mEq of elemental magnesium=99 mg
MgCl =9.8 meq=120 mg
Polymixin B Column for Gram Neg Sepsis
(Crit Care 2005;9:R653)
Anticoagulation
Intensive Care Medicine 2006; 32(2 ):188-202
Final recommendations Risk of bleeding not increased: use UFH (APTT 11.4 times normal) or LMWH (anti-Xa 0.250.35). When systemic anticoagulation is not indicated regional anticoagulation with citrate may be preferred (grade C−). Heparin-induced thrombocytopenia: Stop all kinds of UFH or LMWH (grade C). Use citrate for anticoagulation of the circuit and provide systemic thromboprophylaxis (grade E). The use of danaparoid (anti-Xa 0.250.35 U/ml) can be considered if cross-reactivity with heparin-dependent antibodies is excluded (grade E). The use of hirudin should be discouraged (grade E). Potential alternatives are fondaparinux, bivalirudin, argatroban, dermatan sulfate or nafamostat if monitoring is appropriate (grade E). They need further studies since experience in CRRT is still anecdotal. Risk of bleeding increased: Use regional anticoagulation with citrate (grade C−). CRRT without anticoagulation can be considered, especially with coagulopathy (grade E). Prostaglandins might be considered (grade E). Increased tendency to clotting: The addition of prostaglandins to UFH or LMWH (grade C), the application of predilution (grade C) or the combination of systemic anticoagulation with regional citrate can be considered (grade E).

Sepsis
high-volume CVVH for sepsis: crappy article (Intens Care Med 2006;32:713)
VH and VHD are equivalent for solute removal, except VHD takes longer. Study done using polyacrylonitrile and 35 cc/kg/hr
(Crit Care 2006;10:R67)
Kidney Int. 2006 Oct;70(7):1312-7. Epub 2006 Jul 19. Adding a dialysis dose to continuous hemofiltration increases survival in patients with acute renal failure. These results suggest that increasing the dialysis dose especially for low molecular weight solutes confers a better survival in severely ill patients with ARF.Kidney International (2006) 70, 1312-1317. doi:10.1038/sj.ki.5001705; published online 19 July 2006. Go to source: Entrez PubMed
Can run CVVH without anticoagulation with filter life of ~30 hrs (Inten Care Med 2000;26:1652) require Qb > 200cc/min
Objective The purpose of this study was to evaluate the efficacy and safety of the low molecular weight heparin enoxaparin as anticoagulant in continuous veno-venous hemofiltration (CVVH) compared with unfractionated heparin. Design Prospective randomized controlled crossover study. Setting Medical and Surgical Intensive Care Unit of a University Hospital. Patients Forty consecutive adult medical and surgical ICU patients with normal anticoagulation parameters requiring CVVH. Intervention CVVH was performed with pre-filter fluid replacement at 2500 ml/h and blood flow rates of 180 ml/min. Heparin-treated patients received an initial pre-filter bolus of 30 IU/kg and a maintenance infusion at 7 units/kg h−1, titrated to achieve a systemic activated partial thromboplastin time (aPTT) of 4045 s. Enoxaparin-treated patients received an initial pre-filter bolus of 0.15 mg/kg and a maintenance infusion starting at 0.05 mg/kg h−1, which was subsequently adjusted to maintain systemic anti-factor Xa activity (anti-Xa) at 0.250.30 IU/ml. Each patient received both regimens in a crossover design. Maximum treatment duration for each set was 72 h. Results Patients included had a mean APACHE II score of 22 (1035). Thirty-seven patients completed both study arms. Mean filter life span was 21.7 h (± 16.9 h) for heparin and 30.6 h (± 25.3) for enoxaparin (p = 0.017, ANOVA for repeated measures). One major bleeding episode occurred during heparin as well as during enoxaparin treatment. Cost analysis showed average daily costs of 270 and 240 for heparin and enoxaparin, respectively. Conclusion Enoxaparin can be safely used for anticoagulation during CVVH resulting in higher filter lifespan compared with unfractionated heparin. (Intensive Care Medicine 2007;33(9))
RCT of Citrate shows it is better for filter life (Critical Care 2015, 19:91 )
For Patient in Neurologic ICU from Renal fellow Blog
Based on the above, here are my top tips for a surprise-free existence during your NICU rotation:
1. Choose CVVH if possible
2. Hemodialysis only if stable CV, and no ICP or midline shift:
– Low blood flow rate and cooled dialysate to minimise hypotension
– Small dialyzer to slow the rate of change of plasma osmolality
– High dialysate [Na] (150-160 meq/l)
– Low [bicarbonate] ~ 30 meq/l
– Maintain a pre-dialysis urea of
– Heparin-free
– This is essentially a SLED or hybrid therapy
3. Peritoneal dialysis
– Avoid icodextrin for the same reasons as albumin and mannitol
– Low fill volumes to prevent raised intra-abdominal pressure
Adjacent central venous catheters can result in immediate aspiration of infused drugs during renal replacement therapy
Anaesthesia. 2012 Feb;67(2):115-121
need to be at least 2 cm from arterial port