How Many Tubes do Average ED Docs do and How Many do they Need to
Ann Emerg Med. 2019 Jun 24. doi: 10.1016/j.annemergmed.2019.04.025. [Epub ahead of print]
West J Emerg Med. 2019 Jul;20(4):601-609. doi: 10.5811/westjem.2019.6.42946. Epub 2019 Jul 2.
Skill Proficiency is Predicted by Intubation Frequency of Emergency Medicine Attending Physicians.
Gillett B1, Saloum D1, Aghera A1, Marshall JP1.
Author information
1
Maimonides Medical Center, Department of Emergency Medicine, Brooklyn, New York.
Abstract
Introduction:
Airway management is a fundamental skill of emergency medicine (EM) practice, and suboptimal management leads to poor outcomes. Endotracheal intubation (ETI) is a procedure that is specifically taught in residency, but little is known how best to maintain proficiency in this skill throughout the practitioner’s career. The goal of this study was to identify how the frequency of intubation correlated with measured performance.
Methods:
We assessed 44 emergency physicians for proficiency at ETI by direct laryngoscopy on a simulator. The electronic health record was then queried to obtain their average number of annual ETIs and the time since their last ETI, supervised and individually performed, over a two-year period. We evaluated the strength of correlation between these factors and assessment scores, and then conducted a receiver operator characteristic (ROC) curve analysis to identify factors that predicted proficient performance.
Results:
The mean score was 81% (95% confidence interval, 76% – 86%). Scores correlated well with the mean number of ETIs performed annually and with the mean number supervised annually (r = 0.6, p = 0.001 for both). ROC curve analysis identified that physicians would obtain a proficient score if they had performed an average of at least three ETIs annually (sensitivity = 90%, specificity = 64%, AUC = 0.87, p = 0.001) or supervised an average of at least five ETIs annually (sensitivity = 90%, specificity = 59%, AUC = 0.81, p = 0.006) over the previous two years.
Conclusion:
Performing at least three or supervising at least five ETIs annually, averaged over a two-year period, predicted proficient performance on a simulation-based skills assessment. We advocate for proactive maintenance and enhancement of skills, particularly for those who infrequently perform this procedure.
Best Validated First Pass Success Rate
Systematic review and meta-analysis of first-pass success rates in emergency department intubation: Creating a benchmark for emergency airway careAuthorsFirst published: 27 October 2016Full publication historyDOI: 10.1111/1742-6723.12704View/save citationCited by: 0 articles
Ramp Position is Good for Everyone
DAsH1A
Bill Hinckley elaborated our goal for airway management
Definitive Aiway sine Hypoxemia on the 1st Attempt
Airway Progression
Validation study of the algorithm
Absorption Atelectasis during Preoxygenation
Even preox with 100% did not seem to affect FRC (J Anesth DOI 10.1007/s00540-012-1547-7)
Levitan’s Complexity Article
Complexities of Tracheal Intubation (Ann Emerg Med 2011;57(3):240)
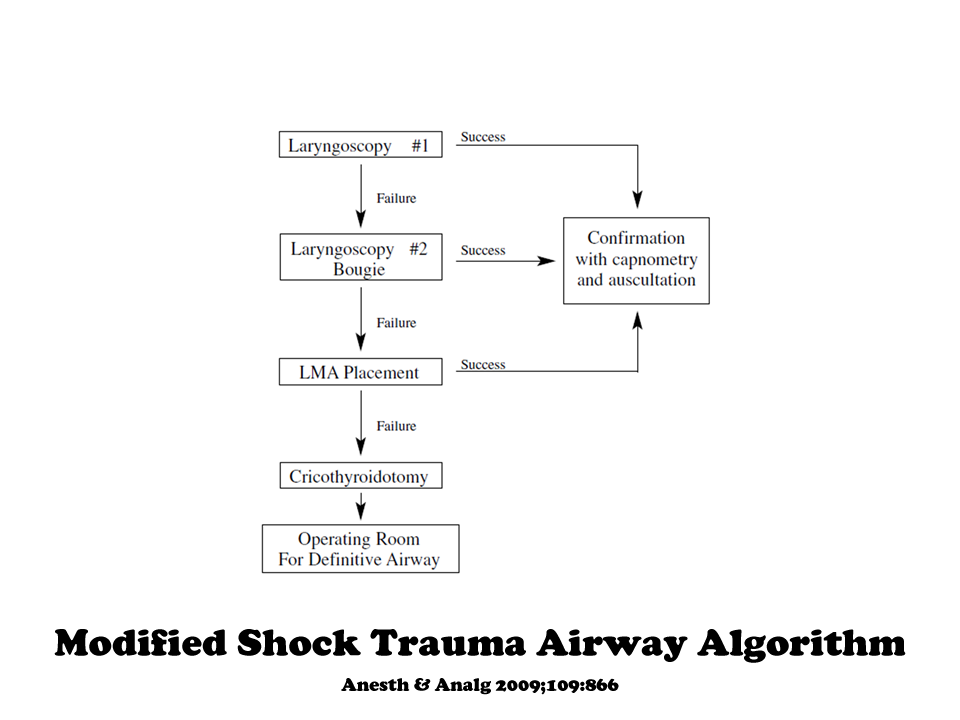
Formulation of a CICO Algorithm
Each Attempt Makes Things Worse
Hasegawa et al. showed at 3 attempts, things got bad (Ann Emerg Med 2012;60:749)
Sackles JC et al. showed that >1 attempt radically increased complications (ACADEMIC EMERGENCY MEDICINE 2013; 20:71–78)
Mort demonstrated this in the ICU, after two attempts risk of crit desat (70%) is huge and assoc. with cardiopulm arrest (Anesth Analg 2004;99:607)
Mort has further elaboration re: the dangers of intubation in the critically ill (J Inten Care Med 2007;22(4):208)
Heffner et al. showed a 4% cardiac arrest rate in ED intubations (Incidence and factors associated with cardiac arrest complicating emergency airway management. Resus 2013)
Duggan showed >1 attempt
{kind=link}
= badness
Cricothyrotomy
Prehospital Meta-analysis (Prehosp Emerg Care 2010;14:515)
Surgical cric is sig. better!
Can we find the membrane with a needle? Not so much (Anaesthesia, 2010, 65, pages 889–894)
Bougie-Aided Cricothyrotomy (Air Medical J 28(4):191

Need for Preoxygenation
If the saturation was 93% or less at the start, the patient is very likely to desaturate and the rapidity of desaturation is predicted by this initial starting sat (Davis PREHOSPITAL EMERGENCY CARE 2008;12:46–51)
Tube Depth
Conclusion Less experienced clinicians should rely more on tube insertion depth than on auscultation to detect inadvertent endobronchial intubation. But even experienced physicians will benefit from inserting tubes to 20-21 cm in women and 22-23 cm in men, especially when high ambient noise precludes accurate auscultation (such as in emergency situations or helicopter transport). The highest sensitivity and specificity for ruling out endobronchial intubation, however, is achieved by combining tube depth, auscultation of the lungs, and observation of symmetrical chest movements. (BMJ 2010; 341:c5943 )
then get a chest xray
Roc Vs. Sux
Same when dosed high (Academic Emergency Medicine Volume 18, Issue 1, pages 10-14, January 2011)
Ketamine-Fentanyl-Roc for prehospital intubations (Lyon. Critical Care 2015; 19:134. doi:10.1186/s13054-015-0872-2)
Better mortality with Roc in TBI? (PMID 26799349)
BVMs cannot be used for Spont Ventilation
They can so long as they don’t have duckbill valves like Mercury Medical. (Fact or Fiction: the patient cannot spontaneously breathe via the bag valve mask apparatus. Arekapudi A., et al. SAM 2012)
Mask Ventilation
When rocuronium was adminsitered compared to placebo, mask ventilation got better (Anaesthesia, 2011, 66, pages 163167)
You need two hands on the mask (One Hand, Two Hands, or No Hands)
Gastric Tubes
My practice is to place gastric tubes prior to intubating GI bleeders or alcoholics. The question is whether this decreases the esophageal sphincter opening pressure
Answer is it doesn’t (Gastroenterology 1976;70:301; Arch Surg 1978;113:721)
Ketamine-Only Intubation
Emerg Med J 2011;28:521 71 Patients, 18 didn’t get paralysis
Injury 1997;28:41
Am J Emerg Med 2007;25:977
Complications of the airway management of the critically Ill
Start worrying at 70%, pt may die below 60% (J Intensive Care Med 2007 22: 208 Mort)
Hemodynamics (J Intensive Care Med 2007 22: 157)
Complications rise at the 3 mor more attempt mark (Anesth Analg 2004;99:60713)
Tube passage attempts are worse than blade passage attempts
Patients who start off on vasopressors have a high risk of peri-intubation codes (Anesthesiol 1995;82:367) and assoc of hypotension post-tube and death (J Crit Care. 2012 Aug;27(4):417)
Most recent study shows a dismally high rate of complications in a French ICU (Early Identification of Patients at Risk for Difficult Intubation in the Intensive Care Unit Am J Respir Crit Care Med. 2013 Apr 15;187(8):832-9)
Prehospital Intubations
Resuscitation. 2011 Apr;82(4):378-85. Epub 2011 Feb 1. Out-of-hospital airway management in the United States. Wang HE, Mann NC, Mears G, Jacobson K, Yealy DM.
Source
Department of Emergency Medicine, University of Alabama at Birmingham, Birmingham, AL 35249, United States. hwang@uabmc.edu
Abstract
OBJECTIVE:
Prior studies describe airway management by single EMS agencies, regions or states. We sought to characterize out-of-hospital airway management interventions, outcomes and complications across the United States.
METHODS:
Using the 2008 National Emergency Medical Services Information System (NEMSIS) Public-Release Data Set containing data from 16 states, we identified patients receiving advanced airway management, including endotracheal intubation (ETI), alternate airways (Combitube, Laryngeal Mask Airway (LMA), King LT, Esophageal-Obturator Airway (EOA)), and cricothyroidotomy (needle and open). We examined airway management success and complications in the full cohort and in key subsets (cardiac arrest, non-arrest medical, non-arrest injury, children
RESULTS:
Among 4,383,768 EMS activations, there were 10,356 ETI, 2246 alternate airways, and 88 cricothyroidotomies. ETI success rates were: overall 6482/8418 (77.0%; 95% CI: 76.1-77.9%), cardiac arrest 3494/4482 (78.0%), non-arrest medical 616/846 (72.8%), non-arrest injury 417/505 (82.6%), children
CONCLUSIONS:
In this study characterizing out-of-hospital airway management across the United States, we observed low out-of-hospital ETI success rates. These data may guide national efforts to improve the quality of out-of-hospital airway management.
and more likely to cause VAP (Eur J Emerg Med 2013;20:61)
Number of Tubes to be Competent
Probably close to 200 (Acta Anaesthesiol Scand 2012; 56: 164–171)
To plateau at 90% success rate took 57 in this study(Anesth Analg 1998;86:635)
Pulse Ox Lag
Latency of up to 120 s has been demonstrated in conditions producing peripheral vasoconstriction (doi:10.1016/j.jemermed.2011.06.127)
Shock Dosing of Sedative Agents
No reduction to get same brain levels of etomidate, 50% for fentanyl, 80-90% for propofol (Anesthesio 2004;101:567)
{kind=link}

Predicting Obstructive Sleep Apnea (OSA)
STOP-Bang Score (Br J Anaes 2012;108(5):768)
Advantages of an awake look using remifentanil (J Clin Anesthesia 2012;24:19)
A clarification on when the crit ill risk of sux kicks in
Anesth Analg. 2012 Jul 4. [Epub ahead of print] The Limits of Succinylcholine for Critically Ill Patients. Blanié A
~16 days
An Abstract demonstrating that with Some Bags–No Spont Breathing
Bougie Use for Trauma MILS Intubation
Less force required with the bougie (Eur J Anaesthesiol 2013; 30:1–4)
Bougie FPS
Ann Emer Med October 2017Volume 70, Issue 4, Pages 473–478.e1
LMA will succeed when Mask and ETI Fail
Parmet et al studied this (Anesth Analg 1998;87:661)
Ultrasound for Difficult Neck Anatomy for Needle Cric
European Journal of Anaesthesiology: July 2011 – Volume 28 – Issue 7 – p 506–510 doi: 10.1097/EJA.0b013e328344b4e1
Higher Height of Table Improves Success
Xiphoid is the ideal height
Higher operating tables provide better laryngeal views for tracheal intubation. (Br J Anaesth. 2013 Dec 18) Lee HC et al. and (Br. J. Anaesth 2014;112 (4):749-755.)
Scissor Maneuver

Intubating the Patient with Head Injury
A clinically significant hemodynamic response to laryngoscopy and intubation is common in patients with head injuries and is not effectively attenuated by increasing head injury severity. The need to attenuate the hemodynamic response should be assessed independently of head injury severity. (J Trauma Acute Care Surg. 2013 Apr;74(4):1074)
Predicting Difficult Intubation
This issue was brilliantly summed up by Yentis in a 2002 Editorial2:
“I dare to suggest that attempting to predict difficult intubation is unlikely to be useful – does that mean one shouldn’t do it at all? To this I say no, for there is another important benefit of this ritual: it forces the anaesthetist at least to think about the airway, and for this reason we should encourage our trainees (and ourselves) to continue doing it.”
1. Diagnostic accuracy of anaesthesiologists’ prediction of difficult airway management in daily clinical practice: a cohort study of 188 064 patients registered in the Danish Anaesthesia Database
Anaesthesia. 2014 Dec 16. doi: 10.1111/anae.12955. [Epub ahead of print]
2. Predicting difficult intubation–worthwhile exercise or pointless ritual?
Anaesthesia. 2002 Feb;57(2):105-9
3. Anaesthesia. 2015 Mar;70(3):272-81.
Diagnostic accuracy of anaesthesiologists’ prediction of difficult airway management in daily clinical practice: a cohort study of 188 064 patients registered in the Danish Anaesthesia Database.
It is Safe to Pull Back Inflated Cuffs
Tracheal rapid ultrasound saline test (T.R.U.S.T.) for confirming correct endotracheal tube depth in children Mark O Tessaro, Evan P Salant, Alexander C Arroyo, Lawrence E Haines, and Eitan Dickman Resuscitation 89:8 (2015) Objective We evaluated the accuracy of tracheal ultrasonography of a saline-inflated endotracheal tube (ETT) cuff for confirming correct ETT insertion depth. DOI: 10.1016/j.resuscitation.2014.08.033 Advertisements
Head Elevation does indeed improve View
Intentional Esophageal Intubation if Massive Vomiting
Time Perception
CMAC is superior to direct for rescue of 1st pass failure
J Emerg Med 2015;48(3):280
Intubation Duration
51-70 seconds in Dutton’s STC RCT (Journal of Trauma and Acute Care Surgery Issue: Volume 75(2), August 2013, p 212–219)
IM Succinylcholine
On the basis of the available evidence, intramuscular administration of succinylcholine at 4 mg/kg may produce muscle relaxation in a timeframe suitable for rapid sequence intubation. This dose consistently produced paralysis in 2 to 4 minutes in infants, children, and adults (Table), with no clinically significant adverse effects in the patients studied. Additionally, intramuscular administration was less arrhythmogenic than intravenous administration (doi:10.1016/j.annemergmed.2015.04.013)
Snail Trail Bougie Bending for Hyperangulated Blades
DOI: 10.1111/anae.13052
{kind=link}

Reflective Intubation Maneuver
{kind=link}

Eur J Anaesth 2015;32:406
How Experts Hold a Laryngoscope compared to Novices
Zamora J et al. Laryngoscope manipulation by experienced versus novice laryngoscopists. Can J Anaesth 2014 Dec; 61:1075
Head-Up Position is Safer and Better
Lane et al. 2005.: ¨Mean (95% CI) apnoea time was 386 (343-429) s in the 20 degrees head-up position (n = 17) vs 283 (243-322) s in the supine position (n = 18; p = 0.002). Pre-oxygenation is significantly more efficacious and by inference more efficient in the 20 degrees head-up position than in the supine position.¨
Ramkumar et al. 2011: ¨Preoxygenation is clinically and statistically more efficacious and by inference more efficient in the 20º head-up position than with conventional technique in non-obese healthy adults. Although application of 5 cmH(2)O PEEP provides longer duration of non-hypoxic apnea compared to conventional technique, it is not statistically significant.¨
Altermatt et al.: ¨Pre-oxygenation in sitting position significantly extends the tolerance to apnoea in obese patients when compared with the supine position.¨
Dixon et al. 2005: ¨Preoxygenation in the 25 degrees head-up position achieves 23% higher oxygen tensions, allowing a clinically significant increase in the desaturation safety period–greater time for intubation and airway control. Induction in the 25 degrees head-up position may provide a greater safety margin for airway control.¨
Boyce et al. 2003: ¨In morbidly obese patients, the 30 degrees Reverse Trendelenburg position provided the longest safe apnoea period when compared to the 30 degrees Back Up Fowler and Horizontal-Supine positions. Since on induction of general anesthesia morbidly obese patients may be difficult to mask ventilate and/or intubate, this extra time may preclude adverse sequelae resulting from hypoxemia. Therefore, Reverse Trendelenburg is recommended as the optimal position for induction.¨
Lee et al. 2007: ¨During laryngoscopy, the laryngeal view, as assessed by POGO scores, improves significantly in the 25 degrees back-up position when compared with the flat supine position.¨
Anesth Analg. 2016 Apr;122(4):1101-7. Head-Elevated Patient Positioning Decreases Complications of Emergent Tracheal Intubation in the Ward and Intensive Care Unit. Khandelwal N1, Khorsand S, Mitchell SH, Joffe AM.
Use Smallest Macintosh you can get away with
Rocuronium Dose affects 1st Pass Success
use greater than or equal to 1.4mg/kg
The Impact of Rocuronium Dose on First-Attempt Intubation Success
Author links open overlay panelN.LevinMD1M.L.FixMD1M.D.AprilMD, DPhil, MSc2A.AranaPhD2T.MadsenMD1A.FantegrossiMPH34C.A.BrownIIIMD34NEAR Investigators
https://doi.org/10.1016/j.jemermed.2020.07.064