Focused Assessment with Sonogram in Trauma
Trauma: The FAST Exam Anywhere from 1-7 views Use sector probe 2-3.5 MHz Each view should take 30-60 seconds
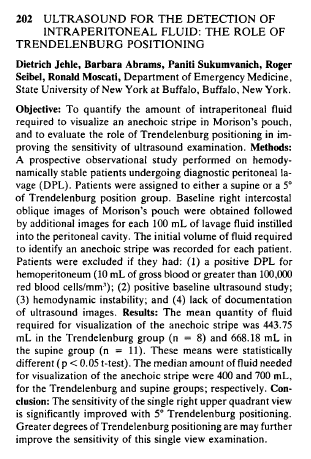
RUQ
Most sensitive view for free fluid in peritoneal space Made more sensitive by scanning in Trendelenburg. 97% sensitivity c 1 L of fluid, 10 % Sensitivity with 400 cc Attempt the scan in sagittal at right midclavicular line moving the probe laterally until kidney/liver interface comes into view. From this position, you can see Morrisons, check for pleural effusion (sensitivity increased with patient flat or in reverse Trendelenburg,) examine paracolic gutters and the liver parenchyma.
If you must scan RUQ in coronal, placing arms over head will open up intercostals spaces. Scan in oblique just off coronal with probe on mid-ax line and indicator pointing towards post-ax line Blood/fluid collections have sharp edges and points b/c it will fill the space between structures. Blood is anechoic, but if there are clots, will be hypoechoic. Liver level signals should be seen on both sides of the diaphragm, if there is an anechoic area opposite liver tissue, it is pleural fluid.
RUQ mean volume required to detect fluid in a dialysis model was 619 cc, at 1 liter, sensitivity was 97%)
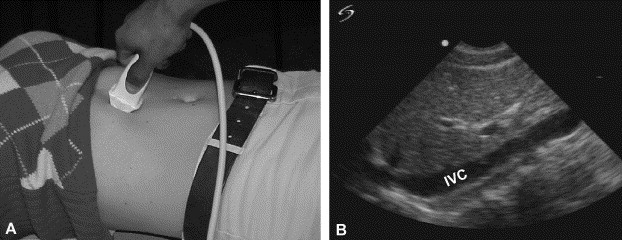
Double-Line Sign
An aritfact of two bright lines with hypoechoic area between. Fascia and fat is what’s is causing the artifact. Fluid next to liver will only have one white line.
The Journal of Emergency Medicine Volume 40, Issue 2 , Pages 188-189, February 2011
Cardiac
Subxiphoid scan c overhand grip. 20-30° off of abdomen aiming at left midclavicular line in transverse orientation with the indicator to patients right (The surgeons do it in sag for some reason). The liver and right ventricle (wedge shaped) will be the first structures seen. They should be in close contact. Anterior fat pad can give false positive, so best if fluid can be seen posterior to left ventricle as well. 
Rozycki Study (J Trauma 1999;46(4):543)
LUQ
Higher than right kidney. Mid axillary line with probe aimed at posterior axillary line. Find kidney then move up until spleen interface is seen. Examine potential splenorenal space for fluid. Scan paracolic gutter, look above diaphragm for pleural effusion, and examine spleen parenchyma for obvious injury (intraparenchymal blood is echogenic), or subdiaphragmatic blood.
false positive:
gastric bubble
Pelvis
The most inferior part of the peritoneal cavity is the pouch of Douglas (cul-de-sac) in women or the Retrovesicular pouch in men. Bladder is the acoustic window, so makes life easier if the FAST is done before foley placement. The bladder will cause acoustic enhancement directly behind it so adjust gain accordingly. First do sagittal to locate bladder and determine level (you must be above prostate or vagina), then turn transverse to evaluate fluid. Women: blood may be seen anterior or posterior to the uterus Men: do not be confused by prostate or seminal vesicles. Look for bowtie sign, fluid on either side of bladder as this is the easiest part for blood to fill.
Pitfalls
· Identification of portal vein or IVC as free fluid · Seminal vesicles as free fluid · Perinephric fat can appear hypoechoic · Anterior fat pad of heart can appear hypoechoic (almost always located anterior to the R ventricle and not behind L ventricle) · Not going posterior enough or high enough on LUQ exam, fingers should touch table · Mistaking ascites for blood. Examine liver for signs of cirrhosis (increased echogenicity, thickened GB wall, splenomegaly)RUQ: Preferably Sagittal showing post. Pleural space, diaphragm, liver, kidney, and Morrisons pouchLUQ: Coronal showing spleen, kidney, diaphragm, posterior pleural space, splenorenal interfaceCardiac: Pericardium, preferably with posterior as well as anteriorSuprapubic: Transverse of bladder showing pouch of Douglas or Retrovesicular space. Must be above the level of the prostate or vagina Include in documentation limited or incomplete study, Dx (Definite, Probable, Possible, Uncertain), and confirmatory study.
Study Study Class Study Size No. of Patients With Hemoperitoneum Sensitivity, % Specificity, % Positive Likelihood Ratio Negative Likelihood Ratio Ma et al 21 I 245 patients 64 90 99 90 0.1 Rozycki et al22 II 1,227 patients 96 83.3 99.7 278 0.17 Shackford et al23 I 241 patients 51 68 98 34 0.33 Smith et al24 III 841 patients 45 73 98 36.5 0.28 Tso et al10 II 163 patients 11 91
(Annals 2004, 43:2 Policy on Blunt Abd Trauma)
Radiology. 2003 Dec;229(3):766-74. Related Articles, Links Screening US for blunt abdominal trauma: objective predictors of false-negative findings and missed injuries. Hematuria and fracture of the lower ribs, lumbar spine, or pelvis are objective predictors of missed abdominal injury in patients with blunt abdominal trauma and negative US findings, and such patients may benefit from additional screening with computed tomography.
IVC
consider cut of of 8 mm for IVCe diameter (expiratory)
(American JEM 2005;23:45)
100% sensitivity for FAST in pts with hypotension
Rozycki GS, Ballard RB, Feliciano DV, Schmidt JA, Pennington SD. Related Articles, Links Surgeon-performed ultrasound for the assessment of truncal injuries: lessons learned from 1540 patients. Ann Surg. 1998 Oct;228(4):557-67.
Sens 97% in radiology study for injuries requiring surgery (Radiology 2005;235:436)
Blaivis case series on using paracentesis to evaluate suspicious fluid found on fast (JEM 2005;29(4):461)
| | |