Western Trauma Association Penetrating Neck Trauma Guidelines 2013
(Journal of Trauma and Acute Care Surgery Issue: Volume 75(6), December 2013, p 936–940)
 from Emerg Med Austalasia
from Emerg Med Austalasia
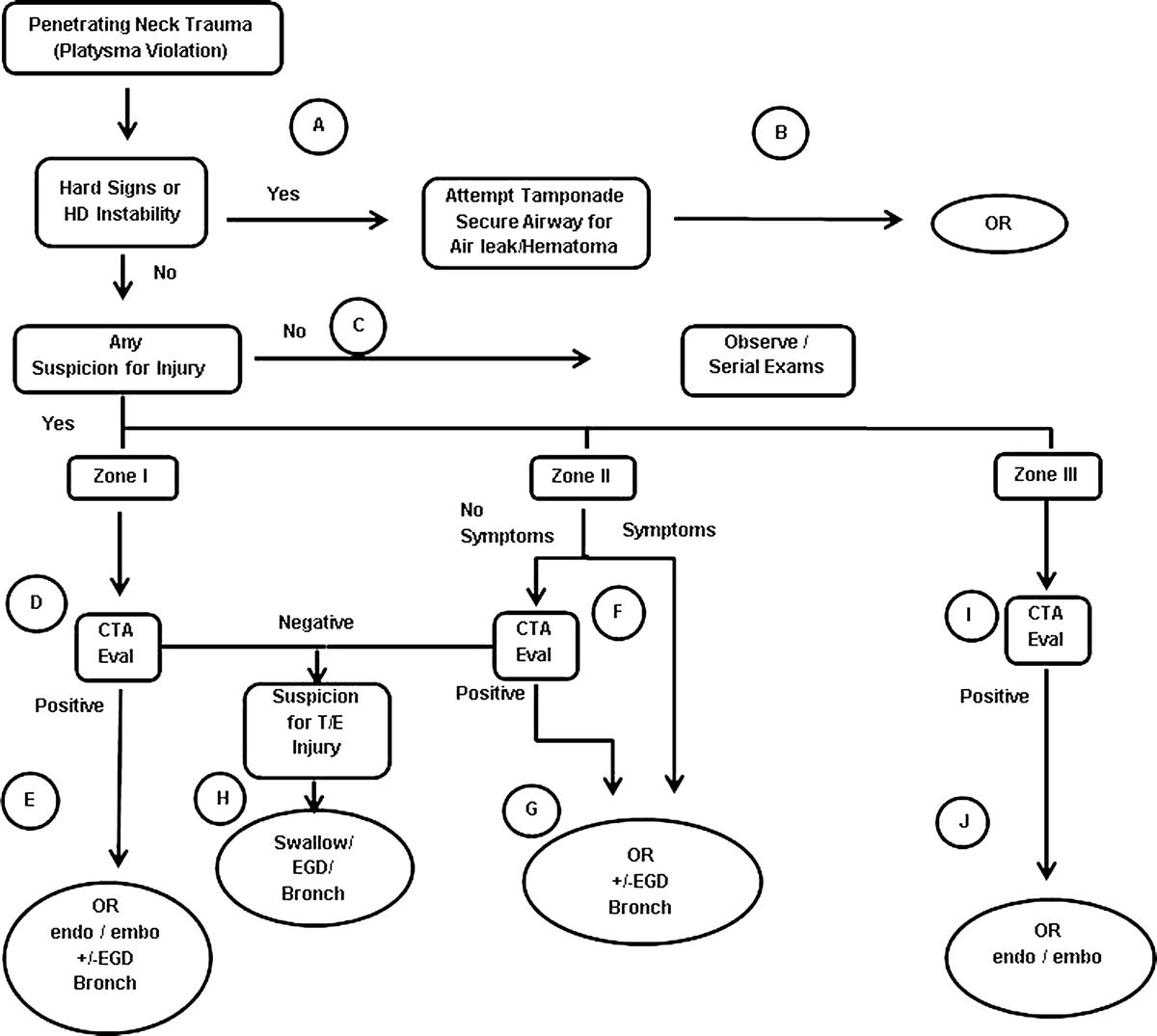
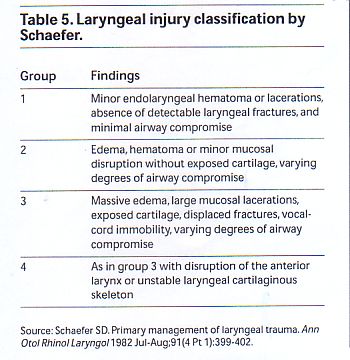
Vascular Injuries, Pharyngoesophageal injuries, or Laryngotracheal injuries.
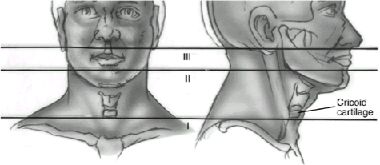
Anterior=forward to sternocleidomastoid
Zone I-below cricoid, angio/esophogram/endoscopy/bronchoscopy
Zone II-between cricoid and mandible. Go to OR
Zone III-above mandible, angio/esophogram/endoscopy/bronchoscopy

If platysma is violated, requires surgical evaluation
Look for Horner’s syndrome (Ptosis, miosis, anhydrosis,
“whooshing” in the ears (pulsatile tinnitus), which is associated with carotid dissection. Pain on swallowing
Esophageal evaluation usually consists of gastrograffin swallow (less pulmonary sequelae than barium), followed by barium, and then endoscopy.
Carducci et al., characteristics of patients requiring immediate exploration include: shock, active bleeding, hematoma (moderate size or expanding), pulse deficit, bruit, neurological deficit, dyspnea, hoarseness, stridor, dysphonia, hemoptysis, subcutaneous emphysema, dysphagia, or hematemasis
can swing the injured external to damaged interna and sacrifice distal external carotid
if patient is stable, consider angiogram
posterior neck wounds
if possible, perform angiogram; there is no easy way to operatively intervene on vertebral injuries
pretracheal fascia is in continuity with the mediastinum
look at articles by Demetriades
Insert foley to tamponade GSW bleeding
Have patient cough, swallow, and speak
mandatory exploration was derived from high velocity injuries during WWII
Munera F, Cohn S, Rivas LA. Penetrating injuries of the neck: use
of helical computed tomographic angiography. J Trauma 2005;58:
413-418.
This article echoes the results of the preceding one. It reviews the
authors’ current protocol for managing penetrating neck injuries, with
specific evaluation of the use of helical CT angiography. The technique
used was administration of nonionic contrast delivered at a rate of 3 to
4.5 mL/s to a total administered volume of 100 mL. Three-dimensional
volume-rendered images were then recreated, which gave the surgeon an
excellent perspective of any lesion viewed from multiple lines of sight. The
authors found that helical CT angiography was 100% sensitive, 98%
specific, and had a predictive value of 93%.
Zone II Clinical Guidelines
Level I: Selective operative management and mandatory
exploration of penetrating injuries to zone II of the
neck have equivalent diagnostic accuracy. Therefore,
selective management is recommended to minimize
unnecessary operations.
Level II: High resolution CT angiography offers appropriate
diagnostic accuracy with minimal risk, making this
the initial diagnostic study of choice when available.
Level III: No recommendations.
Diagnosis of Arterial Injury
Recommendations
Level I: No recommendations.
Level II: CT angiography or duplex US can be used in
lieu of arteriography to rule out an arterial injury in
penetrating injuries to zone II of the neck.
Level III: CT of the neck (even without CT angiography)
can be used to rule out a significant vascular injury if
it demonstrates that the trajectory of the penetrating
object is remote from vital structures. With injuries in
proximity to vascular structures, minor vascular
Diagnosis of Esophageal Injury
Recommendations
Level I: No recommendations.
Level II: Either contrast esophagography or esophagoscopy
can be used to rule out an esophageal perforation
that requires operative repair. Diagnostic workup
should be expeditious because morbidity increases if
repair is delayed by more than 24 hours.
Level III: No recommendations.
Value of the Physical Examination
Recommendations
Level I: No recommendations.
Level II: No recommendations.
Level III: Careful physical examination using protocols
for serial examinations, including auscultation of the
carotid arteries, is 95% sensitive for detecting arterial
and aerodigestive tract injuries that require repair.
Given the potential morbidity of missed injuries, clinicians
should have a low threshold for obtaining
imaging studies.
J Trauma. 2008;64:13921405.
Strangulation Injuries
The literature does not provide specific recommendations as to how to evaluate such patients, in part because presentations are so variable, and because discussions of such injuries often lump hangings and manual strangulation together. It is clear, however, that the severity of traumatic forces that result in significant injury may not be evident on initial examination (1,2,3). Emergency physicians must take seriously any patient who reports a history of recent strangulation injury.
Tardieu Spots and result from the rise in venous pressure in response to the strangulation or ligature tightening.
When a patient presents to the ED in significant distress or with signs and symptoms suggesting a specific injury, the management is often obvious. A standard evaluation algorithm for the patient who is asymptomatic, however, does not exist. Suggested studies for patients that have been strangled include the following: Soft-tissue neck x-rays should be ordered in nearly all strangulation patients. They may demonstrate subcutaneous emphysema (e.g. because of a fractured larynx), fracture of the hyoid bone, or tracheal deviation because of edema or hematoma. CT scan of neck structures. MR of the soft tissues of neck. In addition, gadolinium-enhanced MR angiography can rapidly image the carotid arteries from the aortic arch to the circle of Willis, making it particularly applicable in the setting of blunt cervical injuries where the level of injury is unknown (2). Carotid doppler ultrasound. Duplex evaluation is being used increasingly as a screening tool in patients with blunt neck trauma, although angiography remains the gold standard for diagnosing blunt carotid artery injury (2). There are anecdotal reports using helical CT scans to demonstrate blunt carotid artery injuries, but future studies are needed to validate its efficacy. Laryngosocopy. Vocal cord and tracheal evaluation, especially in patients with dyspnea, dysphonia/hoarseness, odynophagia Precisely how the array of available studies are to be used and which patients warrant an extensive work-up if they are without signs and symptoms is not clear. Since specific protocols are lacking, it might be illuminating to note how a minimally symptomatic strangulation victim was managed in actual practice at a level 1 trauma center. The patient depicted on the preceding page underwent soft tissue films of the neck, CT imaging of his larynx and MRA to evaluate for possible carotid injury. All of the studies were negative and he was discharged home. He had no delayed injuries noted in follow-up examination. One interesting point: Behavioral changes in patients who have been strangled are important to note, but are often dismissed as a psychological in origin given the stress of the attack. Behavioral changes may manifest early as restlessness and combativeness because of temporary anoxia and subsequently resolve. Victims have been reported to die days or even several weeks later because of progressive, irreversible encephalopathy (1). References: (1) McClane GE, et al. A Review of 300 Attempted Strangulation Cases, Part II: Clinical Evaluation of the Surviving Victim J Emerg Med 2001; 21: 311-315 (2) Kumar SR Cervical vascular injuries: carotid and jugular venous injuries Surg Clin North Am 2001; 81: 1331-44 (3) Marx: Rosen’s Emergency Medicine: Concepts and Clinical Practice, 5th Edition, Copyright 2002 Mosby, Inc.
- Soft-tissue neck x-rays should be ordered in nearly all strangulation patients. They may demonstrate subcutaneous emphysema (e.g. because of a fractured larynx), fracture of the hyoid bone, or tracheal deviation because of edema or hematoma.
- CT scan of neck structures.
- MR of the soft tissues of neck. In addition, gadolinium-enhanced MR angiography can rapidly image the carotid arteries from the aortic arch to the circle of Willis, making it particularly applicable in the setting of blunt cervical injuries where the level of injury is unknown (2).
- Carotid doppler ultrasound. Duplex evaluation is being used increasingly as a screening tool in patients with blunt neck trauma, although angiography remains the gold standard for diagnosing blunt carotid artery injury (2). There are anecdotal reports using helical CT scans to demonstrate blunt carotid artery injuries, but future studies are needed to validate its efficacy.
- Laryngosocopy. Vocal cord and tracheal evaluation, especially in patients with dyspnea, dysphonia/hoarseness, odynophagia
HCTA for neck trauma instead of angio:
70. Mazolewski PJ, Curry JD, Browder T, et al. Computed tomographic scan can be used for surgical decision making in zone II penetrating neck injuries. J Trauma 2001 Aug;51(2):315-319. (Prospective; 14 patients)
71.* Munera F, Soto JA, Palacio D, et al. Diagnosis of arterial injuries caused by penetrating trauma to the neck: comparison of helical CT angiography and conventional angiography. Radiology 2000 Aug;216(2):356-362. (Prospective; 60 patients)
72. LeBlang SD, Nunez DB, Rivas LA, et al. Helical computed tomographic angiography in penetrating neck trauma. Emerg Radiol 1997 July/Aug;4(4):2-206. (Prospective; 35 patients)
10 yr experience with hangings (Injury 2006;37:435) SBP<90, GCS<8, Anoxic brain injury, ISS>15
only anoxia on ct was independent.
Patients with any signs of life may regain full function
There is considerable misunderstanding about the neck injury in hanging, including the notion that radical displaced fractures occur. Fracture of cervical vertebrae C2 and C3 (the hangmans fracture), alleged to occur in judicial hanging, relates to the force applied by dropping the body some distance, against a ligature applied from the side of the neck (30). In suicidal hanging, as opposed to judicial hanging, there is rarely a drop of the body. Most suicidal hangings are accomplished while standing or kneeling. A common misconception is that there will be fractures or some sort of internal neck injury in people who hang themselves. In fact, in suicidal hanging there is scarcely ever any internal evidence of neck injury at all (5,7,10). Suicidal hanging is usually effected with very little force. It is painless, and can be accomplished even when lying down in bed. External injury, including the dramatic rope burns or ligature abrasion, only occurs after the body has been suspended for several hours after death. If the ligature is released at the moment of death, there will be no mark on the skin. After the body has hanged suspended by the ligature for a few hours, a very dramatic furrow and ligature abrasion will develop post-mortem. Immediate death from hanging or strangulation can progress from one of four mechanisms:
1. Cardiac dysrhythmia may be provoked by pressure on the carotid artery nerve ganglion (carotid body reflex) causing cardiac arrest.
2. Pressure obstruction of the carotid arteries prevents blood flow to the brain.
3. Pressure on the jugular veins prevents venous blood return from the brain, gradually backing up blood in the brain resulting in unconsciousness, depressed respiration, and asphyxia.
4. Pressure obstruction of the larynx cuts off air flow to the lungs, producing asphyxia.
The first mechanism (carotid body reflex) is very uncommon. The reflex cardiac dysrhythmia can be reproducibly demonstrated in humans, but force must be applied over a very localized and specific anatomic area. The second mechanism (carotid arterial obstruction) is also very uncommon in suicidal hangings, but may be more frequent in homicidal strangulations. Quite a bit of pressure is required to obstruct arterial flow in the carotids, and that amount of force typically would be associated with obvious soft tissue injury locally in the neck. The third mechanism (jugular venous obstruction) is probably the usual route for death by suicidal hanging. Slight pressure fully or at least partially obstructs venous return bilaterally in the internal and external jugular veins, gradually causing passive congestion of blood in the vessels within the brain. Note that this mechanism is different from surgical ligation or surgical sacrifice of one of the four jugular veins, typical of radical neck surgery. Partially obstructing return in all four veins diminishes oxygen delivery to the brain, eventually resulting in loss of consciousness. The type of pressure required is slight, but prolonged. Unconsciousness probably doesnt occur for several minutes, but the overall process is completely painless. In cases of suicidal hanging, eventually the individual becomes unconscious, then the fourth mechanism (laryngeal obstruction) takes over. With the person unconscious, the full weight of the suspended part of the body falls against the ligature, creating enough pressure to restrict air flow through the trachea. Then, irreversible asphyxiation follows in just a few minutes. In strangulation cases, and some suicidal hangings where the individual is saved before death, there may be a prolonged period of survival with obvious brain damage, followed by death. This delay is the effect of loss of blood flow to the brain, with partial asphyxiation of the brain. A decrease in blood flow to the brain will produce a pathologic change called anoxic encephalopathy. Brain cells are not all equally sensitive to loss of blood flow. Some cells die soon, while others survive for days and eventually succumb to the delayed effect of oxygen deprivation. Nerve cell death may be patchy in the brain. The nerve cells of the hippocampus and dentate nucleus, and Purkinje cells of the cerebellum, are more susceptible to anoxia than cortical nerve and glial cells. Fatal anoxic encephalopathy results in clinical brain death where the body functions of the heart and internal organs can be maintained by medical life support, but all hope of meaningful recovery is lost. Complications may include persistent vegetative coma, cerebral edema (brain swelling), and herniation of the brain. For patients who do recover consciousness, lifelong brain damage may be observed. Quantitating the actual forces applied to the neck is not a meaningful exercise. The amount of force required to compress the jugular veins is less than the force to compress the carotids, and that in turn is less than the force required to constrict the airway. However, absolute valuesmeasured as foot-pounds of forcevary tremendously from one person to the next depending on development of neck musculature, and the surface area for the application of force. If the force were applied over a very narrow surface areaa clothesline ligature as opposed to a broad belt, for examplethen much less force would be necessary. Four variables are working simultaneously, as shown in Figure 7. For the same amount of pressure, if you decrease the surface area, or increase the duration of the force, you increase the likelihood that the force will be fatal. Further, if even a small force is applied in just the right 320 D. A. Hawley et al. anatomic area, the force may obviate the normal anatomic protections of the neck musculature and skeleton. A small woman can easily strangle a large man. Medical resuscitation, and organ procurement procedures, work against the pathologists ability to detect fatal homicidal neck injury (12). An oxygen mask can leave abrasions on the mouth and nasal bridge. During resuscitation, an airway tube is placed into the mouth or nose, and inserted into the esophagus or trachea, to establish a path through which air can be forced under pressure to the lungs. The usual airway device is an oral endotracheal tube, but many varieties of hardware exist. The skill of the rescue staff, and the size and rigidity of the victim, dictate how much injury occurs during this intubation procedure. Traumatic intubations result in internal injuries of the deep musculature of the larynx, often completely mimicking the injuries of strangulation. Ulceration of the larynx may develop from pressure produced by the inflatable cuff on the tube. The mechanical ventilation can produce barotrauma in the lungs, with air dissecting up to the skin of the neck. In cases where the rescue staff is unable to intubate the patient, they may attempt a surgical cricothyrotomy or tracheostomy procedure to establish an airway. This may completely obliterate all signs of manual strangulation. Further, IV needles are sometimes placed into the jugular veins, leaving tracks of hemorrhage that can obscure physical injuries. If resuscitation is successful, the patient may linger on mechanical ventilation for hours or days, resulting in healing of soft tissue injuries in the neck
The Journal of Emergency Medicine, Vol. 21, No. 3, pp. 317322, 2001
if doing swallow, start with gastro, then barium. is paradigm in some centers but this makes no sense. gastrograffin has no place in these studies
Barium bad for belly and mediastinum. Gastro bad for the lungs
British Study of Omnipaque, Ultravist, and Hexabrix (iso-oncotic) safe and accurate as single agent for swallow (Emerg Med J 2009;26:106)
Another retrospective review (J Trauma 2009;66:174) GCS has no absolute predictive value.
Zone IV Injuries
ZONE IV OF THE NECK?: TEN-YEAR EXPERIENCE WITH PENETRATING TRAUMA TO THE POSTERIOR NECK There were 757 patients with a penetrating neck injury, of which 224 (30%) had a posterior neck wound. Gender ratio was 89% male to 11% female. Mechanism was 60% GSW, 30% SW, 3% SGW, and 7% other or combined. 44 (20%) patients had neck exploration, 31 (70%) positive and 13 (30%) negative. Angiography was performed on 72 (32%) patients, 23 (32%) positive and 49 (68%) negative. Mortality rate was 14/224 (6%), all but one death from GSW. CONCLUSIONS: Emphasis on clearance of the cervical spine should be a component of the early management of penetrating trauma to the posterior neck. A distinct diagnostic algorithm for these injuries may be warranted.
Tracheobronchial Injury
if pt crashes right after intubation, consider air embolism. Put pt in LLR/trendelenberg. If you cross clamp the hilium of injured side and aspirate the ventricle, you may save a life.
pt’s with small defects and no other serious injuries may be managed non-op using PEEP and low tidal volumes
injuries need to be small (<1/3 of tracheal circumference) and aymptomatic (J Trauma 2005;59(5):1075)

Inaba did the largest evaluation of MDCTA to date (The Journal of Trauma and Acute Care Surgery Volume 72(3), March 2012, p 576–584) CTA is accurate, attending physical exam can obviate the need for the CTA in the first place. If exam shows no signs of vascular or aerodigestive injury at all, imaging may be able to be avoided.