Penetrating Abdominal Trauma
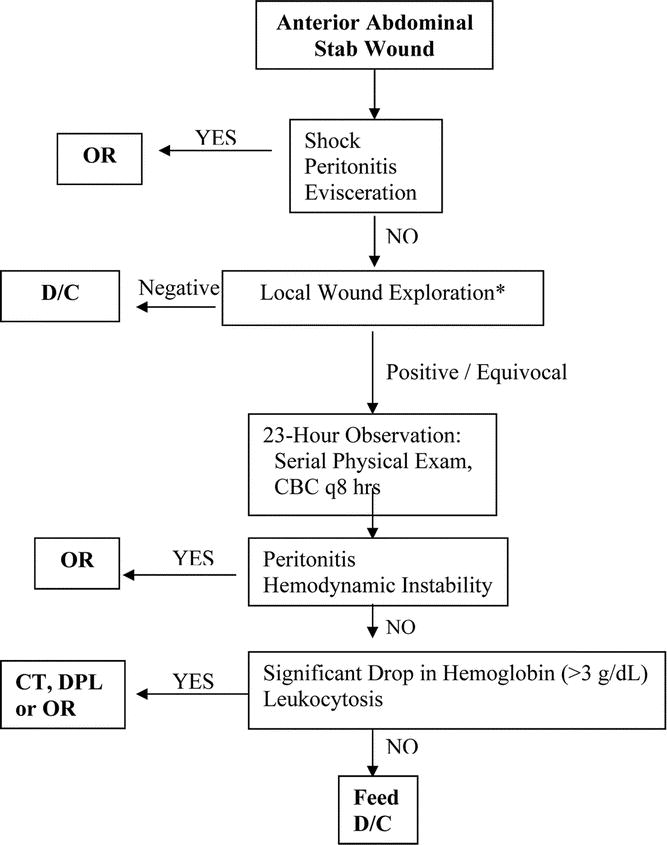
The WEST’s review of the management of anterior stab wounds
(J Trauma Volume 66(5), May 2009, pp 1294-1301) and then the validation
( J Trauma 2011;71(6)1494)
1494")
DPA sens 89% spec 100% (Int J Surg 2007;5(3):167)
May be safe to discharge AASW after 12 hours (J Trauma 2005;58:523)
EAST Pen Abd Trauma Guidelines (excerpted from Resus.me)
- Patients who are hemodynamically unstable or who have diffuse abdominal tenderness should be taken emergently for laparotomy (level 1).
- Patients who are hemodynamically stable with an unreliable clinical examination (i.e., brain injury, spinal cord injury, intoxication, or need for sedation or anesthesia) should have further diagnostic investigation performed for intraperitoneal injury or undergo exploratory laparotomy (level 1).
- A routine laparotomy is not indicated in hemodynamically stable patients with abdominal stab wounds (SWs) without signs of peritonitis or diffuse abdominal tenderness (away from the wounding site) in centers with surgical expertise (level 2).
- A routine laparotomy is not indicated in hemodynamically stable patients with abdominal gunshot wounds (GSWs) if the wounds are tangential and there are no peritoneal signs (level 2).
- Serial physical examination is reliable in detecting significant injuries after penetrating trauma to the abdomen, if performed by experienced clinicians and preferably by the same team (level 2).
- In patients selected for initial nonoperative management, abdominopelvic CT should be strongly considered as a diagnostic tool to facilitate initial management decisions (level 2).
- Patients with penetrating injury isolated to the right upper quadrant of the abdomen may be managed without laparotomy in the presence of stable vital signs, reliable examination, and minimal to no abdominal tenderness (level 3).
- The majority of patients with penetrating abdominal trauma managed nonoperatively may be discharged after 24 hours of observation in the presence of a reliable abdominal examination and minimal to no abdominal tenderness (level 3).
- Diagnostic laparoscopy may be considered as a tool to evaluate diaphragmatic lacerations and peritoneal penetration (level 2).
J Trauma. 2010 Mar;68(3):721-733
Most Recent Review of LWE for AASW (AM J Surg 2009;198:223)
If doing non-op management of GSW, 24 hours is in-patient obs time (J Trauma Volume 68(6), June 2010, pp 1301-1304)
Probing of Abd stab wounds specific, but insensitive (Annals of EM)
| | |