Best Review
NEJM 2013;369(9):840 Angus et al.
For More Great Evidence and Resources on Sepsis, See our Sepsis Collaborative Page at EMCrit.org
Review of all current lit (Annals Emerg Med 2006;48(1):28)
Loma Linda Toolkit from
Nguyen
ICU Sepsis Screen

Sepsis Definitions
Systemic Inflammatory Response Syndrome (SIRS)
The hallmark clinical manifestations of both sepsis and SIRS are two or more of the following conditions:
1. Temperature 38ºC or 36ºC
(100.4/96.8)
2. Tachycardia 90 beats per minute 3. Respiratory rate 20 per minute or a PaCO2 32 mm Hg 4. White blood cell count 12,000 mm3 or 4,000/mm3 or 10% immature (band) forms (“left shift”). SSC Criteria Infection plus any two, get lactate Temp 101 or 96.5 Altered Mental Status Chills with Rigors Tachy 90 RR 20 WBC 12000 or 4000 Sugar 120 mg/dl in absence of diabetes signs of severe sepsis, any of the following distinct from the source of infection SBP 90 or MAP 65 or SBP decrease 40 from baseline Cr 2.0 or UO 0.5 cc/kg/hour Billi 2 mg/dl PLT 100,000 Lactate 4 INR 1.4 or PTT 60 bilat infiltrates with criteria for ALI or need for increased supplemental O2 to maintain SpO2 90
Sepsis
2 or more SIRS plus infection
from the ancient Greeks, who used ?sepsis? to describe putrefaction and a bad smell
Severe Sepsis
Sepsis c organ dysfunction, hypoperfusion, hypotension, AMS, acidosis, oliguria, ARDS
Septicemia
pathogens in the blood stream
Septic Shock
Hypotension after 2L of fluid
ARDS
PaO2/FiO2 200
B pulmonary infiltrates
PAWP 18
Bone’s criteria define septic shock as systolic BP 90 mm Hg or 40-mm drop in standard BP; organ perfusion based on mean arterial BP, which is determined by diastolic, not systolic, BP; patients whose BP usually 170/100 mm Hg who present with BP of 110/60 mm Hg have septic shock (ie, 40-mm Hg drop in baseline BP; do not treat with fluids); precipitous drop in mean arterial BP causes change in mental status, hemodynamic embarrassment, renal dysfunction, gastrointestinal (GI) tract hypoperfusion, and liver hypoperfusion (DeBlieux)
Types of Hypoxia
hypoxemic hypoxia (low paO2)
Anemic Hypoxia
Stagnant Hypoxia (low CO)
Cytopathic Hypoxia (Cell machinery can not use O2)
Who has Severe Sepsis?
Infection plus any two, get lactate
- Temp 101 or 96.5
- Altered Mental Status
- Chills with Rigors
- Tachy 90 RR 20
- WBC 12000 or 4000
- Sugar 120 mg/dl in absence of diabetes
signs of severe sepsis, any of the following distinct from the source of infection
- SBP 90 or MAP 65 or SBP decrease 40 from baseline
- Cr 2.0 or UO 0.5 cc/kg/hour
- Billi 2 mg/dl
- PLT 100,000
- Lactate 4
- INR 1.4 or PTT 60
- bilat infiltrates with criteria for ALI or need for increased supplemental O2 to maintain SpO2 90
Fluids in Sepsis
In early sepsis, we pour in the fluids as proven by EGDT studies
AFter the resus period, fluid management is very different
Pts have a normal or supranormal oxygen delivery. Even after fluids and blood, pts may have decreased MAPs; the temptation is to keep administering fluids, but this is often counterproductive.
Fluids can be harmful:
Normal ICU care gives patients a ton of extraneous fluid already–med infusions
 Figure 1 Cardiac output (CO) [and, similarly, venous return] depend on Pra. However, this relationship depends critically on where the heart is operating on its function curve. For example, when the heart is at point A, small increments in Pra raise cardiac output greatly.
Figure 1 Cardiac output (CO) [and, similarly, venous return] depend on Pra. However, this relationship depends critically on where the heart is operating on its function curve. For example, when the heart is at point A, small increments in Pra raise cardiac output greatly.
In contrast, augmenting Pra when the heart is at point B has little impact on cardiac output.
 Figure 2. Venous return function curve superimposed on the cardiac function curve. For this heart, the current state is described by the intersection point of the cardiac function and venous return function curves (arrow 1). Raising mean systemic pressure (for example, by infusing fluids or raising the legs) shifts the venous return function curve rightwards. The new state (higher Pra and higher cardiac output) is represented by the new intersection point (arrow 2).
Figure 2. Venous return function curve superimposed on the cardiac function curve. For this heart, the current state is described by the intersection point of the cardiac function and venous return function curves (arrow 1). Raising mean systemic pressure (for example, by infusing fluids or raising the legs) shifts the venous return function curve rightwards. The new state (higher Pra and higher cardiac output) is represented by the new intersection point (arrow 2).
Dynamic Measures
Spont inspiration will transiently raise the transmural Pra and shift CO curve to the left, increasing CO
Passive Mech Vent Inspiration shifts the CO curve to the right and temporarily decreases CO
 Figure 3. The effect of spontaneous breathing is to shift leftwards the cardiac function curve (solid line to dotted line), shifting the intersection point from arrow 1 (end-expiration) to arrow 2 (end-inspiration). When the heart is operating on the steep portion of the cardiac function curve (top, a), this leftward shift moves the intersection point significantly (ie, Pra falls and cardiac output rises). However, if cardiac function is depressed or the circulation is fluid loaded (bottom, b), the respiratory shift (from arrow 1 to arrow 2) has only a trivial impact on Pra and cardiac output.
Figure 3. The effect of spontaneous breathing is to shift leftwards the cardiac function curve (solid line to dotted line), shifting the intersection point from arrow 1 (end-expiration) to arrow 2 (end-inspiration). When the heart is operating on the steep portion of the cardiac function curve (top, a), this leftward shift moves the intersection point significantly (ie, Pra falls and cardiac output rises). However, if cardiac function is depressed or the circulation is fluid loaded (bottom, b), the respiratory shift (from arrow 1 to arrow 2) has only a trivial impact on Pra and cardiac output.
 Figure 4. Passive ventilation shifts the cardiac function curve rightwards. The solid line represents end-expiration (intersection point 1), and the dotted line end-inspiration (intersection point 2). If the heart is preload responsive (top, a), the intersection point shifts and the resulting decrease in cardiac output will reveal itself in changing pulse pressure, stroke volume, and aortic or brachial artery peak flow velocity. If the heart is not preload responsive (bottom, b), there will be little respiratory-related decrease in cardiac output (as the intersection point shifts from arrow 1 to arrow 2).
Figure 4. Passive ventilation shifts the cardiac function curve rightwards. The solid line represents end-expiration (intersection point 1), and the dotted line end-inspiration (intersection point 2). If the heart is preload responsive (top, a), the intersection point shifts and the resulting decrease in cardiac output will reveal itself in changing pulse pressure, stroke volume, and aortic or brachial artery peak flow velocity. If the heart is not preload responsive (bottom, b), there will be little respiratory-related decrease in cardiac output (as the intersection point shifts from arrow 1 to arrow 2).
 Figure 5. Relationship of arterial pressure wave and passive respiration. Compared to end-expiration, the systolic pressure and pulse pressure rise during inspiration (INSP), then fall during expiration. PPmax = maximal pulse pressure; PPmin = minimal pulse pressure.
Figure 5. Relationship of arterial pressure wave and passive respiration. Compared to end-expiration, the systolic pressure and pulse pressure rise during inspiration (INSP), then fall during expiration. PPmax = maximal pulse pressure; PPmin = minimal pulse pressure.
Recommendations for Fluid Management in Severe Sepsis For the first 6 h of severe sepsis, infuse fluids liberally, targeting SvO2 or ScvO2 70% Subsequently, do not use “maintenance” fluids Judge the intravascular volume daily (at least) For new hypotension, tachycardia, or unexplained oliguria, ascertain the cause and consider a fluid challenge: When fluid challenge is of low risk, administer 500 to 1,000 mL of crystalloid; When the risk of fluid challenge is not trivial (ALI/ARDS; oliguria; right ventricular dysfunction), use a dynamic predictor to guide fluid boluses PLR for those with some measure of cardiac output; PPV for those with regular rhythm and lack of spontaneous breathing; Change in Pra for those with substantial inspiratory effort Reassess the patient frequently because the hemodynamic state changes often
Table 3. How To Measure PPV* Check that cardiac rhythm is regular Raise the tidal volume to 10 mL/kg of predicted body weight Ensure that the patient is receiving ventilation passively or adjust further the rate, tidal volume, or degree of sedation to achieve this Display or print the arterial pressure waveform for 30 s Measure the minimum and maximum pulse pressure Calculate PPV (PPmax ? PPmin)/([PPmax + PPmin]/2) x 100% A value 13% predicts fluid responsiveness
* See Figure 5 legend for expansion of abbreviations.
A Bedside Approach
We summarize here our recommendations for management of fluids in septic patients (Table 2 ). In the first 6 h of acute resuscitation, fluids should be infused urgently to restore perfusion, guided by the ScvO2. Although infusing fluid until the Pra reaches 8 to 12 mm Hg is commonly recommended, the only basis for this is expert opinion.1281 We are concerned that excessive focus on Pra will lead to underresuscitation or overresuscitation, emphasize again that ScvO2 should be the target, and recommend that dynamic predictors be used (even at this early time) to gauge the likely impact of fluids.
Once the patient has been resuscitated, fluid infusion should be ceased and no maintenance fluids should be prescribed. The intravascular and total body volume state should be judged periodically (daily in a rather stable patient, more frequently in the newly admitted or unstable patient) using conventional means such as clinical examination, intake and output records, changes in weight, adequacy of urine output and perfusion, and other measures. Generally, such assessment should be followed by diuretic administration because the typical septic patient is hypervolemic. When persistent or recrudescent hypotension, tachycardia, or oliguria raise the question as to whether fluids would be helpful, the intensivist should estimate the probability of harm from a fluid bolus. For many patients, the risks of fluid expansion are trivial and, in such a case, an adequate fluid bolus should be infused rapidly while measuring clinically relevant outcomes. For others, however, the risks of fluid infusion may be real. Pulmonary or cerebral edema, abdominal compartment syndrome, acute right-heart strain, or oliguria are all conditions that raise the potential risk. Especially when these conditions are present, the clinician should attempt to identify patients unlikely to benefit from fluids, in order to spare them potential harm. Depending on the monitoring available (arterial line, PAC, ScvO2, echocardiography, Doppler ultrasound), one of the dynamic predictors of fluid responsiveness should be used to guide any fluid therapy. Most often this will involve PPV, as described in Table 3 . Technology is available to display PPV, but care must be taken that the preconditions for reliable measurement are adhered to (passive patient, tidal volume of 8 to 12 mL/kg, regular rhythm). The patient must be assessed carefully for respiratory activity, taking into account the ventilator pressure and flow waveforms, hemodynamic tracings, and the clinical examination. We recommend that the arterial pressure wave be printed on paper, preferably along with measures of airway pressure or chest volume, for careful assessment and measurement of pulse pressures. Visually and with the aid of a ruler, we find the tallest and shortest pulse waves, ensuring that these represent the typical cyclic pattern in a long strip. Further, it is essential to be certain that the cardiac rhythm remains regular, especially when choosing values of minimum and maximum pulse pressure. We then simply measure the pulse heights in millimeters on a ruler because there is no need to perform the arithmetic in millimeters of mercury. The equation for calculating PPV is provided in Table 3.32 If the PPV is 13%, a fluid bolus should be administered. Some reliable indicator of perfusion should be measured before and after the bolus in order to determine the effect. If the bolus is effective, the patient should be assessed again for fluid responsiveness, and the procedure repeated until dynamic measures predict no further response. If the initial bolus is not effective, the intensivist should ask whether this is because the bolus was inadequate or the patient is simply unresponsive to fluid.
Article I have no idea what to with about positive fluid balance, uncontrolled for a billion variables (Crit Care Med 2011;39:259) did the patients have heart dysfunction giving high cvp, did they have kidney dysfunction leading to positive fluid balance
Albumin
Intensive Care Medicine
Volume 37, Number 1, 86-96, DOI: 10.1007/s00134-010-2039-6
Original
Impact of albumin compared to saline on organ function and mortality of patients with severe sepsis
The SAFE Study Investigators
and SR/MA (Crit Care Med 2011;39:386)
Vasopressors in Septic Shock
Xigris (Protein C)
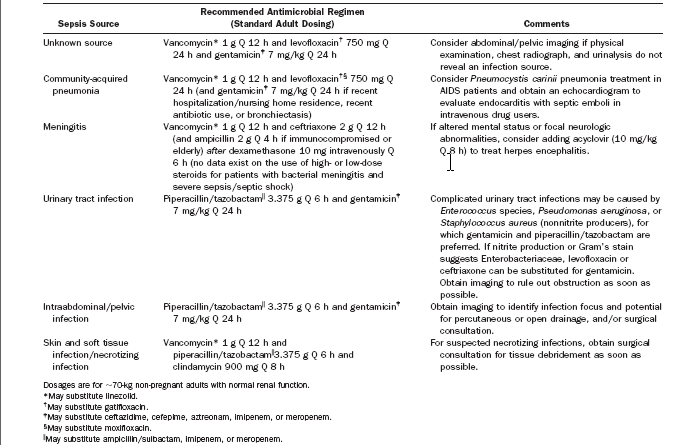
Antibiotics
Retrospective study showed 6% absolute mortality benefit to pts who received abx that covered the bugs within 60 minutes (Crit Care Med 2006;34:1589)
 time to abx from outset of hypotension is assoc with mortality
time to abx from outset of hypotension is assoc with mortality
Elapsed times from triage and qualification forearly goal-directed therapy to administration of appropriate antimicrobialsare primary determinants of mortality in patients withsevere sepsis and septic shock treated with early goal-directedtherapy. (Crit Care Med 2010; 38:1045?1053)
(Chest. 2009 Nov;136(5):1237-48)Initiation of inappropriate antimicrobial therapy results in a fivefold reduction of survival in human septic shock. Kumar
When other varaibles are controlled for, the actual pathogen or infection site doesn’t seem to matter, only getting appropriate abx in early (Crit Care Med 2011;39:1886)
Resuscitation Endpoints
Trends of vital signs are not sufficient endpoints to determine an adequate response to therapy. Rady et al114 showed that 31 of 36 patients presenting with shock and resuscitated to normal vital signs continued to have global tissue hypoxia, as evidenced by decreased ScvO2 and increased lactate levels. A post hoc analysis of the early goal-directed therapy study5 in patients with mean arterial pressure greater than 100 mm Hg showed that control patients with persistently abnormal ScvO2 and lactate levels at 6 hours had a significantly higher mortality rate compared with the early goal-directed therapy patients whose values had reached therapeutic goals (60.9% versus 20.0%, P .05).122 Other studies have also showed that a persistently high lactate is associated with increased mortality.74, 77, 123 and 124 Therefore, continuous ScvO2 and serial lactate measurements during resuscitation may help identify patients requiring continued intensive therapy.
114 114 M.Y. Rady, E.P. Rivers and R.M. Nowak, Resuscitation of the critically ill in the ED responses of blood pressure, heart rate, shock index, central venous oxygen saturation, and lactate, Am J Emerg Med. 14 (1996), pp. 218?225. SummaryPlus | Full Text + Links | PDF (850 K) | Abstract + References in Scopus | Cited By in Scopus
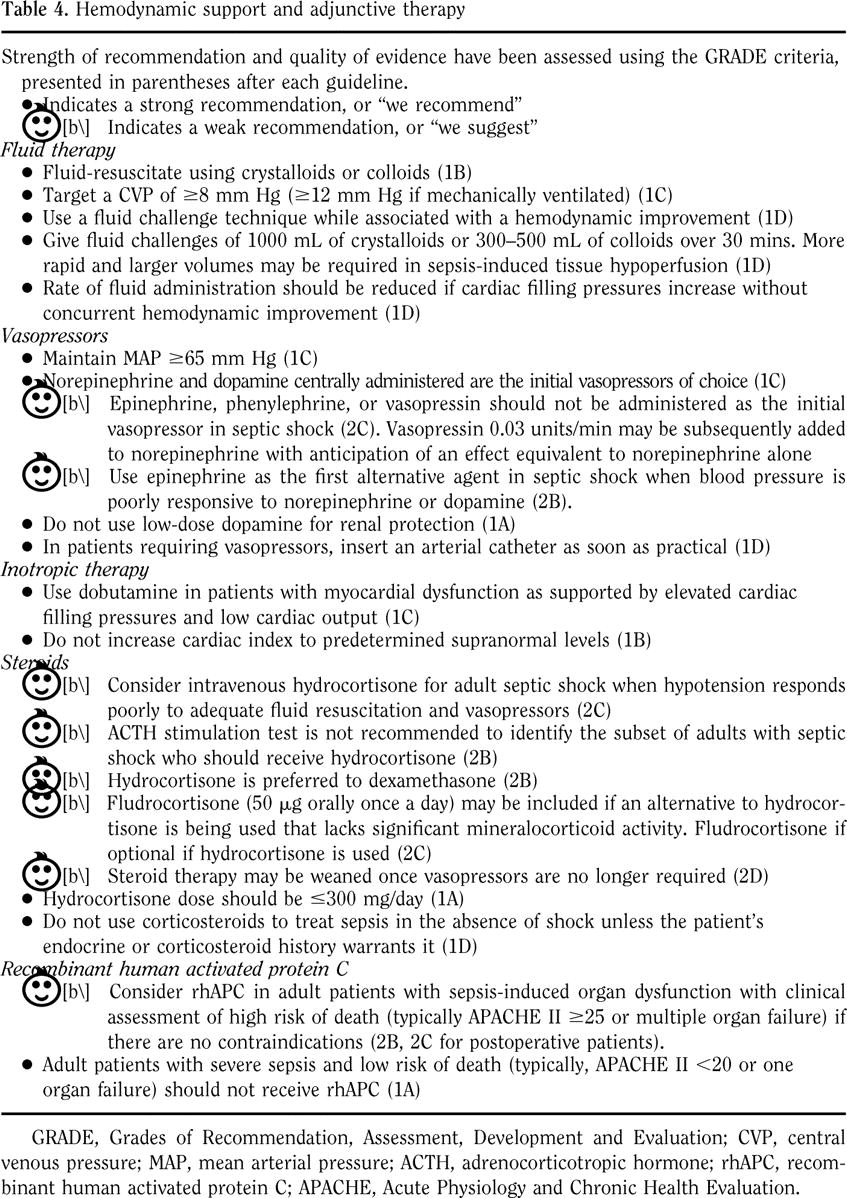
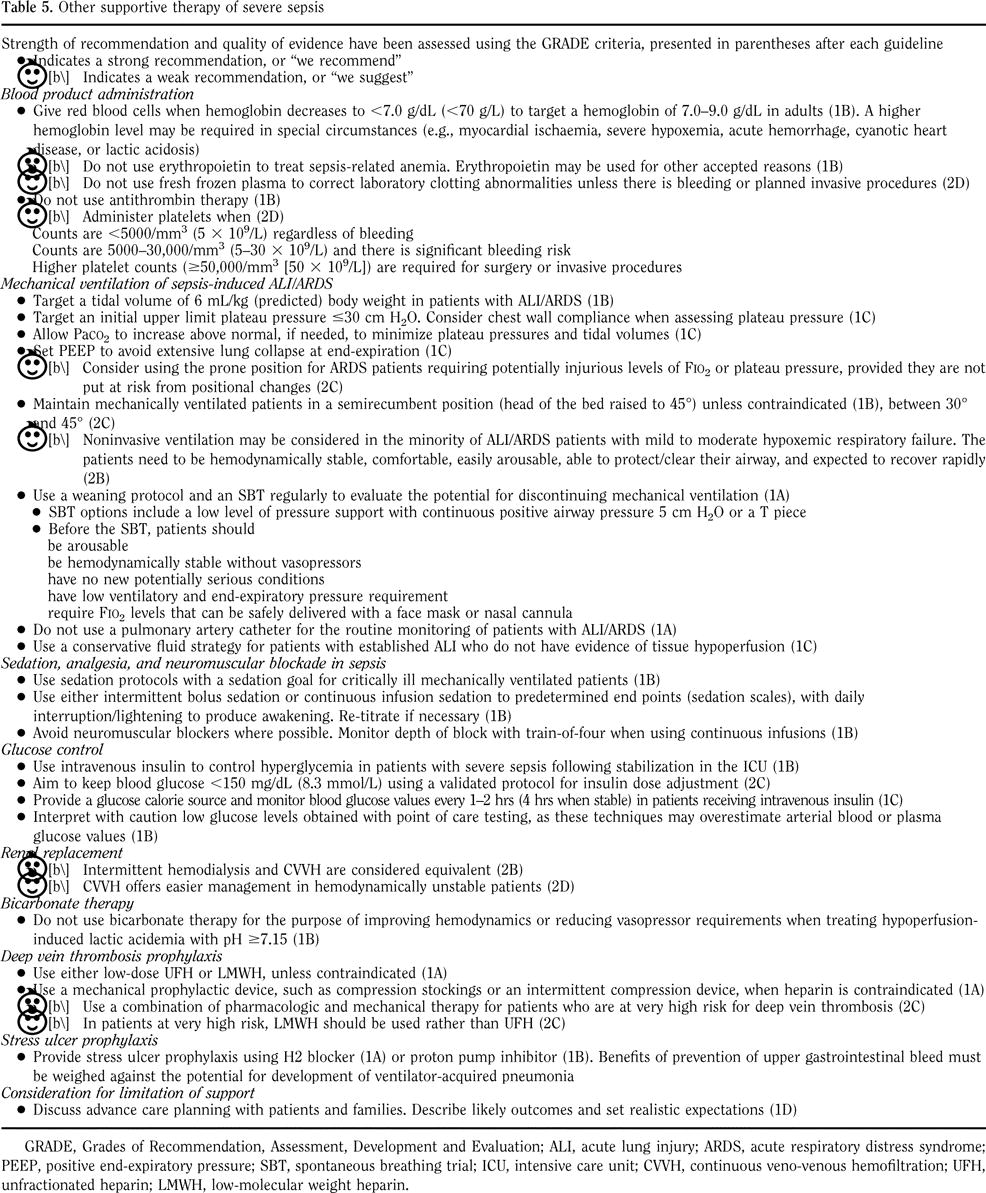
Surviving Sepsis Campaign Guidelines
Critical Care Medicine Volume 36(1), January 2008, pp 296-327
Surviving Sepsis Campaign Explanations (Crit Care Med 2004;32(11) suppl Nov 2004)

Steroids & Adrenal Insufficiency
Statins
correct microcirculatory flow abnormalities through Statins in the intensive care unit. Curr Opin Crit Care. 2006 Aug;12(4):309-14 Association of statin therapy and increased survival in patients with multiple organ dysfunction syndrome. Intensive Care Med. 2006 Aug;32(8):1248-51. Statins and sepsis. Lancet. 2006 May 20;367(9523):1651
Review
Brit J Anaes 2007;98(2):163
Lactate
Serum Lactate as a Predictor of Mortality in Emergency Department Patients with Infection (Ann of Emerg Med 2005;45(5):524-528)
Early lactate clearance assoc c decreased mortality and apache II (crit care med 2004;32(8):1637)
Blueprint for Sepsis (Acad Emerg Med 2005;12(4):352)
Lactate Predicts Death in Emergency Department Patients with Infection
Nathan I. Shapiro, Larry A. Nathanson, Michael Howell, Daniel Talmor, Alan Lisbon, Richard E. Wolfe and J. Woodrow Weiss
Beth Israel Deaconess Medical Center: Boston, MA
CONCLUSIONS: The serum lactatelevel shows initial promise as a predictor of death in patientswith infection, and may be useful as a risk stratification tool.Continued enrollment and the addition of clinical variableswill assist in risk assessment. Further study is necessary todetermine if early lactate-guided intervention can alter outcome.
As lactate increases from 2.0 to 8.0, mortality increases from 10-90% (Crit Care Med 1992;20:80)
venous and arterial is essentially equivalent in the ed population (Acad Emerg Med 1996;3:730)
but another article (1: Ann Emerg Med. 1997 Apr;29(4):479-83) suggests only real if low.
Lactate predicts death regardless of shock/organ failure (Crit Care Med Volume 37(5), May 2009, pp 1670-1677)
Even Lactates between 2-4 were predictive of mortality (Crit Care Med 2009 Vol. 37, No. 5,1670)
Now even 0.75 may be bad (Critical Care 2010, 14:R25)
point of care lactate improves pts getting goal-directed therapies (Am J Resp Crit Care 2010;181:A6141)
Shock. 2009 Jul;32(1):35-9. Multicenter study of early lactate clearance as a determinant of survival in patients with presumed sepsis. 79% of pts who didn’t clear their lactate had an ScvO2 70
Less severe sepsis progresses to severe sepsis with some regularity (Acad Emerg Med 2010;17:383)
Point-of-Care fingerstick lactate seems accurate enough to use for screening (West J Emerg Med 2013;14(1):58)
StO2
The prognostic value of muscle StO2 in septic patients (Intensive Care Medicine 2007;33(9))
Early Goal Directed Therapy
River’s Study (NEJM 345:19 11/8/01)
RCT?263 Patients Post-ED Blinded Control=”Standard Care” ARR Mortality 16% NNT=~6 Patients
follow-up with rationale (Chest 2006;130:1579)
Also benefited post-op major surgery pts, though not in mortality (Crit Care 2005;9:R687)
Nguyen Retrospectively reviewed the feasibility of EGDT, steroids, and Xigris (Acad Emerg Med 2006;13(1):109)
Mortality benefit proven again by Trzeciak 1 year experience with egdt (Dellinger Chest 2006;129(2):225)
22 patients with 16 historical controls. Mortality rate 43% in pre group `8% in EGDT but not stat sig.
before and after review (Crit Care Med 2006;34:2707)
and another (Crit Care Med 2006;34:943)
Bryant’s How to get it done (Acad Emerg Med 2007;14:1079)
Economics
$5000 less per patient due to decreased LOS (Shorr AF. CCM 2007;35(5) POLF)
More on it costing less (Crit Care Med 2007;35:1257) and (35:2090)=Dave Huang’s
In another study, not cost-saving, but cost effective given QALY saved (Crit Care Med 2008;36:1168)
Jones showed it costs more but cost effective with QALY (Crit Care Med 2011;39:1306)
River’s Protocol
If SIRS and SBP 90 or Lactate 4
- Central venous catheter capable of measuring central venous oxygen saturation (ScvO2)
- A-Line
- 500-mL bolus of crystalloid every 30 minutes to achieve a CVP of 8-12 mm Hg
- Vasopressors or vasodilators to achieve MAP 65 mm Hg or 90 mm Hg, respectively
- If ScvO2 was 70%, patients received red blood cell transfusions to achieve a hematocrit of at least 30%.
- If at that hematocrit, ScvO2 was still 70%, patients were infused an escalating dose of dobutamine to a maximum dose of 20 mcg/kg/min.
- Patients then unable to achieve goals were intubated and ventilated
nguyen’s study (Crit Care Med 2007;35(4):1105) if entire bundle, mortality benefit
If using SvO2, 65% should be the target. (CCM Volume 32(7) July 2004 pp 1627-1628)
another prospective validation (Chest 2007;132:425)
intermittent sampling seems almost as good as cont. (Inten Care Med 2007;Online first Author Sakka SG)
(Chest. 2007 Aug;132(2):425-32)
CONCLUSIONS: Implementation of EGDT in our ED was associated with a 9% absolute (33% relative) mortality reduction. Our data provide external validation of the clinical effectiveness of EGDT to treat sepsis and septic shock in the ED.
New meta-analysis of “quantitative” therapies for sepsis showed benefit if early but none if done late. (Crit Care Med 2008;36:2734)
We should probably add on ScvCO2-SaCO2 6 as a marker for need for further resus after ScvO2 70 (Inten Care Med 2008;34:2218)
ScvO2 64 indicated CI 2.5 in an observational trial (Acta Anaes Scand 2010 54:98)
Low and High ScvO2 correlated with mortality (Ann Emerg Med 2010;55(1):40)
Can go non-invasive using 10% lactate clearance instead of ScvO2 in RCT JAMA 2010;303(8):739
More before and after shows ScvO2 70 actually has mortaliy benefit (Crit Care Med 2010 Vol. 38, No. 4)
Prognosis
Early changes in organ function predict survival
(Crit Care Med 2005;33(10):2194)
if you are not getting better, you are getting worse
baseline to day 1 improvement is the best predictor of outcome
MEDS Score
MEDS Score Crit Care Med 2007;35:192 Crit Care Med 2003;31:670 MEDS score was better than APACHE II for predicting mortality (Emerg Med J 2006;23:281-5)
Validated in SIRS patients (Crit Care Med 2008;36:421?6 )
Performance:
SIRS did not improve mortality but severe sepsis or septic shock did (Ann Emerg Med 2006;48:583)
Mottling Score

Fig. 1 Left: the mottling score is based on a mottling area extension on the legs.
- Score 0 indicates no mottling;
- score 1, a modest mottling area (coin size) localized to the center of the knee;
- score 2, a moderate mottling area that does not exceed the superior edge of the kneecap;
- score 3, a mild mottling area that does not exceed the middle thigh;
- score 4, a severe mottling area that does not go beyond the fold of the groin;
- score 5, an extremely severe mottling area that goes beyond the fold of the groin.
Six hours after inclusion,
oliguria [OR 10.8 95% CI (2.9, 52.8), p = 0.001],
arterial lactate level [ 1.5 OR 1; between 1.5 and 3 OR 3.8 (0.7-29.5); 3 OR 9.6 (2.1-70.6), p = 0.01] and
mottling score
0-1 OR 1;
score 2-3 OR 16,
score 4-5 OR 74,
were strongly associated with 14-day mortality
(Intensive Care Med. 2011 May;37(5):801-7)
Equipment
Additional Equipment for EGDT (Crit Care 2005;9:349)
Physiology of Sepsis
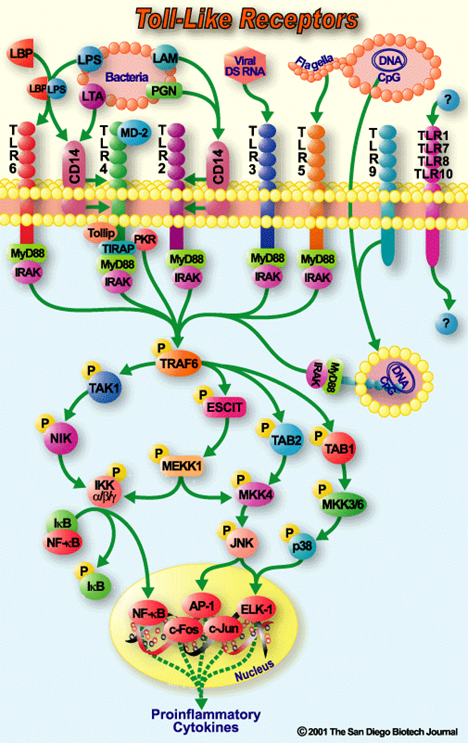

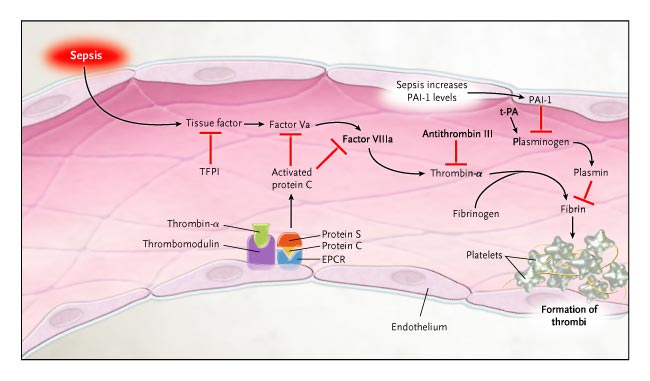
Predisposition Predisposition to respond to therapy genetic comorbidities, environmental, social ie alcohol Infection Factors that may affect prognosis and likelihood of response to therapy identifiable infection source, severity, localized-disseminated (eg bacteraemia) organisms, appropriate/inappropriate initial antimicrobial therapy Response stratification of response based on: biomarkers conventional laboratory parameters eg WBC, procalcitonin, CRP, lactate Organ dysfunction number of organ dysfunctions specific organ dysfunctions magnitude of each organ dysfunction Levy MM, Fink MP, Marshall JC, et al. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit Care Med 2003; 31:1250-1256 PIRO After an infectious insult, endothelial damage occurs. Activation of neutrophils increased vascular permeability with resulting tissue edema liberation of oxidants by the neutrophil. Tissue factor (TF) is expressed by monocytes and the damaged vascular endothelium Inflammatory cytokines, such as tumor necrosis factor (TNF)-alpha and interleukin (IL)-1 and IL-6, are secreted by the monocytes Coagulation activation finally release of thrombin and the formation of the fibrin clot ?Walling off? infection Immune system overstimulation is not central Cytokines may actually be beneficial in sepsis Innate immune cells initiate responses via the Toll Like Receptors (TLR) TLR 4 is part of a recognition complex for bacterial lipopolysaccharide Modulation of tissue TLRs during the early phases of polymicrobial sepsis correlates with mortality Activation of nuclear factor kappaB a transcription factor involved in immediate early gene activation during inflammation Williams DL, Ha T, Li C, et al. Modulation of tissue Toll-like receptor 2 and 4 during the early phases of polymicrobial sepsis correlates with mortality. Crit Care Med 2003; 31:1808-1818 Hotchkiss RS, Karl IE. The pathophysiology and treatment of sepsis. N Engl J Med 2003; 348:138-150
Mental status changes ? ANY KIND Confusion/delirium/compativeness Your pleasant grandpa is now pulling his lines out Decreased responsiveness, pt is less perky Lethargy Tachypnea and/or tachycardia WITHOUT fever (yet) Hypothermia ? remember RECTAL temperature Dropping (slightly initially) blood pressure ? beware of RELATIVE changes Your hypertensive granny with a BP of 100/82 may very well be septic Rising blood sugar ? increasing insulin requirements
Cardiac Dysfunction
? from circulating factors tnf, IL 1b
intrinsic cellular alterations
nitric oxide induced mitochondrial damage
depressed contractility with preserved or initially increased CO
dobutamine may help~15% of pts initially
septic cardiomyopathy
recovers at day 7-10 with no lasting damage
(inten care med 2006;32:799)
~60% of patients have sepsis induced hypokinesia (Crit Care Med 2008;36:1701)
Dobutamine assoc. with increased mortality in a propensity analysis (Acta Anaesthesiologica Scandinavica Volume 57, Issue 4, pages 431–442, April 2013)
Source Control
Does the patient have a correctable source anywhere in his body? Abscess Liver Brain Retroperitoneum Lung-mediastinum Could the pleural effusion be an empyema? Can the dilated kidney represent an obstructive pyelonephritis? Are the paranasal sinuses/teeth filled with pus? Is there any dead bowel in the abdomen? Is the ascites infected? Is the hematoma infected? Is the gallbladder infected? Has this organ perforated?
Sublingual Capnometry
predicts microcirculatory changes and dobutamine reverses these changes in early sepsis (Intensive Care Medicine 2006;32:516)
shunting from stiffened endothelium closes down the microcirc. Increased cardiac output opens it back up
Opening the Microcirculation
Any pt with sepsis and some evidence of organ dysfunction derives mortality benefit from aggressive early therapies (Critical Care 2005, 9:R607-R622)
MEDS Score mortality in ed sepsis score (Crit Care Med 2003;31(3):670)
Economics of EGDT protocol. This study states it is cheaper for the ED or hospital (Crit Care Med 2007;35:1257)
sepsis timeline by Bryant (AJEM 2007;25:564)
Corticus
Bottom line: Hydrocortisone does not help in septic shock
European DB PRCT, 52 ICUs
1º outcome target decreased 28 day mortality in non-responders to ACTH ( 9 rise)
2º outcome targets ICU and hospital mortalities, reversal of organ failures
Planned enrolment 800 patients to give a 80% power to detect a 10% reduction in mortality. Only 500 patients enrolled.
Inclusion Infection within 72 hours
2+ SIRS criteria
Evidence of shock despite fluids and vasopressors
Organ dysfunction
ACTH test required
Exclusion Prior steroids or immunosuppression
Dose of hydrocortisone: 50mg qid x4 days, 50mg bid x 3days, 50 mg once daily for 3 days
35 % of patients were medical
Source of infection was GI 49%, lungs 30%,
Non response to ACTH in 47% both groups
28 day mortality Steroid Placebo All patients 33.5% 31% ns Responders 28.8% 28.7% ns Non-responders 37.6% Missed it but ns difference
Steroid Placebo Reversal of shock 80% 74.6% p=0.14 Median time to reverse shock – all patients 3.1 days 5.7 days p=0.003 Median time to reverse shock – non-responders 3.7 days 6 days Median time to reverse shock – responders 2.8 days ? Secondary superinfection 33% 26.3% was sig ICU neuropathy 1% 2% RR 0.5 (0.09-2.68) Hyperglycemia 150 84% 72% RR 1.17 (1.06-1.28)
Conclusions: Hydrocortisone does not decrease mortality in septic shock
Does not increase reversal of shock but shock reverses quicker
No polyneuropathy increase
More superinfection
ACTH is test not useful
Hydrocortisone should not be routinely used in septic shock.
There may be a role in those still hypotensive after 1 hour. I’ve no idea why they suggest this.
VASST
Vasopressin in Septic Shock Trial
Bottom line; mortality decreased with low dose vasopressin only in patients with less severe sepsis
1º hypothesis – Low dose vasopressin -0.03units/min will decrease 28 day mortality from 60% to 50% in septic shock compared to norepinephrine alone
2º stratification – Severe septic shock = norepinephrine dose 15 mcg/min
Less severe septic shock = norepinephrne 5-14 mcg/min
Resulted in 50% in each group
Inclusion Severe septic shock
SIRS criteria 2/4
Infection
1 organ dysfunction
Exclusion Septic shock 24h, unstable heart, had received any vasopressin
Method Blinded infusion of vasopressin 0.01units/min or norepinephrine 5mcg/min
Titrated to MAP 65-75 mmHg
If vasopressin reached 0.03units/min or norepi 15mcg/min then other pressors were added
Results 396 randomised to vasopressin, 382 to norepi, all were equally sick with 2.5 organ failures and were on 20mcg/min norepi
Measured vasopressin was very low in the noprepi group and 80-100picomol/L in the vaso group
28 day mortality Norepi Vasopressin p value Total 39.3% 35.4% 0.26 More severe sepsis 42.5% 44% 0.84 Less severe sepsis 35.7% 26.5% 0.04
90 day mortality, I couldn’t write the numbers fast enough, but overall the difference in mortality was not significant p= 0.11 but the less severe sepsis group had a mortality of 46.1% with norepi, and 35.8% with vasopressin which was significant at p=0.04.
BP was similar in both groups
No difference in adverse events in both groups except small increase in digital ischemia in the vaso group with p= 0.06
SSC Campaign Results
Data from 15,022 subjects at
165 sites were analyzed to determine the compliance with bundle
targets and association with hospital mortality. Compliance with the
entire resuscitation bundle increased linearly from 10.9% in the first
site quarter to 31.3% by the end of 2 yrs (p .0001). Compliance
with the entire management bundle started at 18.4% in the first
quarter and increased to 36.1% by the end of 2 yrs (p .008).
Compliance with all bundle elements increased significantly, except
for inspiratory plateau pressure, which was high at baseline. Unadjusted
hospital mortality decreased from 37% to 30.8% over 2 yrs
(p .001). The adjusted odds ratio for mortality improved the longer
a site was in the Campaign, resulting in an adjusted absolute drop of
0.8% per quarter and 5.4% over 2 yrs (95% confidence interval, 2.5?8.4).
Conclusions:
The Campaign was associated with sustained,
continuous quality improvement in sepsis care. Although not
necessarily cause and effect, a reduction in reported hospital
mortality rates was associated with participation. The implications
of this study may serve as an impetus for similar improvement
efforts. (Crit Care Med 2010; 38:367?374)
Pentastarch and Intensive Insulin
(NEJM 2008;358(2):125) Intensive Insulin Therapy and Pentastarch Resuscitation in Severe Sepsis Background The role of intensive insulin therapy in patients with severe sepsis is uncertain. Fluid resuscitation improves survival among patients with septic shock, but evidence is lacking to support the choice of either crystalloids or colloids. Methods In a multicenter, two-by-two factorial trial, we randomly assigned patients with severe sepsis to receive either intensive insulin therapy to maintain euglycemia or conventional insulin therapy and either 10% pentastarch, a low-molecular-weight hydroxyethyl starch (HES 200/0.5), or modified Ringer’s lactate for fluid resuscitation. The rate of death at 28 days and the mean score for organ failure were coprimary end points. Results The trial was stopped early for safety reasons. Among 537 patients who could be evaluated, the mean morning blood glucose level was lower in the intensive-therapy group (112 mg per deciliter [6.2 mmol per liter]) than in the conventional-therapy group (151 mg per deciliter [8.4 mmol per liter], P 0.001). However, at 28 days, there was no significant difference between the two groups in the rate of death or the mean score for organ failure. The rate of severe hypoglycemia (glucose level, 40 mg per deciliter [2.2 mmol per liter]) was higher in the intensive-therapy group than in the conventional-therapy group (17.0% vs. 4.1%, P 0.001), as was the rate of serious adverse events (10.9% vs. 5.2%, P=0.01). HES therapy was associated with higher rates of acute renal failure and renal-replacement therapy than was Ringer’s lactate. Conclusions The use of intensive insulin therapy placed critically ill patients with sepsis at increased risk for serious adverse events related to hypoglycemia. As used in this study, HES was harmful, and its toxicity increased with accumulating doses. (ClinicalTrials.gov number, NCT00135473 [ClinicalTrials.gov] .)
Blood
analysis from SOAP study seems to show no increased mortality in pts receiving blood transfusions (Anesthes 2008;108:31)
Barriers to Implementation
National survey of ED directors and nursing directors (CCM 2007;35 POLF Carlbom DJ)
Infection + any two, get lactate
Temp 101 or 96.5
Altered Mental Status
Chills with Rigors
Tachy 90
RR 20
WBC 12000 or 4000
Sugar 120 mg/dl in absence of diabetes
signs of severe sepsis, any of the following distinct from the source of infection
SBP 90 or MAP 65 or SBP decrease 40 from baseline
Cr 2.0 or UO 0.5 cc/kg/hour
Billi 2 mg/dl
PLT 100,000
Lactate 4
INR 1.4 or PTT 60
bilat infiltrates with criteria for ALI or need for increased supplemental O2 to maintain SpO2 90
Intubation for ScvO2
Intubating will increase the ScvO2 if it is low (Impact of emergency intubation on central venous oxygen saturation in critically ill patients: a multicenter observational study Critical Care 2009, 13:R63)
Digoxin in Sepsis
Digoxin at a dose of 10 mcg/kg IV over 3 minutes may have a strong inotropic response for septic patients (Chest 1989;95:612)
measured maximum response in a 6 hour period
Heme Stable Sepsis Patients progress to Badness
(Acad Emerg Med 2010;17:383)
StO2
ScvO2 kinda matches but not so much StO2
(Acad Emerg Med 2010;17:349)
Femoral ScvO2 does not correlate with Neck ScvO2
CHEST July 2010 vol. 138 no. 1 76-83
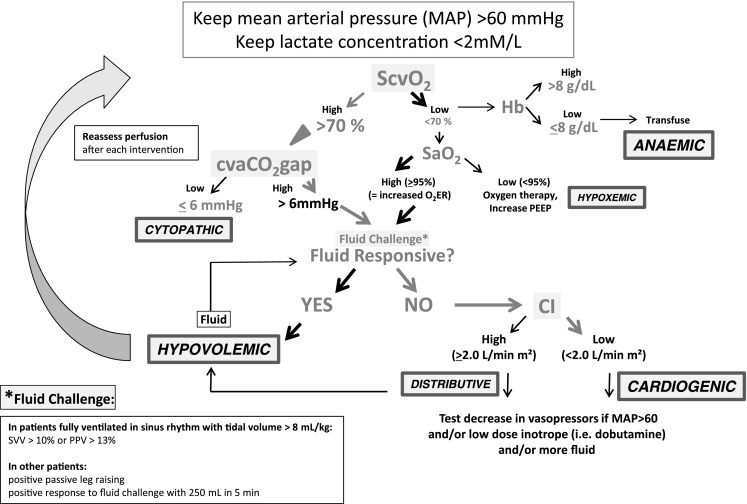
CO2 A/V for ScvO2 70
intra-op optimization using ScvO2 and Art/Ven CO2 differencePcv-aCO2 decreased tissue blood flow (tissue hypoxia) causes increased values for this marker 6 mmHg seems to be cut-off in this trialCO2 stagnation phenomenonCritical Care 2010, 14:R193
The difference between the central venous/mixed CO2 and the arterial is the CO2 gap; it may be a surrogate of Cardiac Output.
Vallet et al. created a protocol (Intens Care Med 2013;39:1653):
Sepsis Care in Resource Limited Environments
Monitored Care in Uganda (Crit Care Med 2012;40:2050)
Procalcitonin
[Emergency Medicine Literature of Note: on JAMA & Procalcitonin]
and
http://www.emlitofnote.com/2013/05/falling-short-on-pneumonia-prediction.html
High Flow CRRT
High Dose CRRT in yet another study did not pan out ( Intensive Care Medicine September 2013, Volume 39, Issue 9, pp 1535-1546 )
Vasoplegic vs. Tissue Dysoxic Septic Shock
they definitely seem to be different states (Shock 2013;40;1:11)