Traumatic tap 1 WBC:750 RBC (Roberts and Hedges)
Tests to order:
Cell Count
Chemistries (Glucose, Protein)
Culture/Gram Stain
Latex Agglutination (If gram stain negative with suspicion)
Cytology-if suspicion of tumor
Fungal/AFB/Crypto/VDRL if immunocompromised
If you suspect crypto, get opening pressures and closing pressures
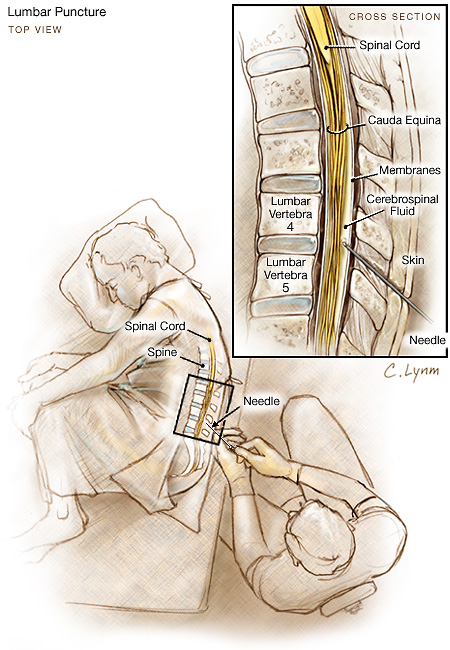
A measurement of opening pressure should be attempted, unless the patient is so uncooperative as to invalidate the reading. CSF pressure should be measured with the subject in the horizontal lateral decubitus position (as described previously) and relaxed as much as possible. Normal range is 80-180 mm H 20, with small, visible excursions related to respiration and pulse. In cases of extremely high pressure (eg, 730 mm H20) the smallest sample possible (for the required testing) should be removed, followed by consideration of CSF pressure-lowering treatment, with continuous monitoring of the pressure until it decreases significantly.
Lateral approach
locate the mid point of the interspace between the dorsal spinous processes, then dropping laterally 1 cm, and caudally 1 cm. (for ease of wrist angle on insertion, it is easier if the lateral “drop” is downward toward the table with the patient lying flat on his side in the usual position) Then angle the needle 45 degrees cephalad and 45 degrees toward the midline. This allows you to “go around” the dorsal spinous processes and enter the dura at the base of the spinous processes. Recognize that this approach traverses a bit more territory so the needle hub is going to be closer to the skin when you enter the dura. You can do this also with the patient in the sitting position (useful in very obese patients when you are having difficulty palpating the dorsal spinous processes and need some extra help even finding the mid-line).
LP safe in kids with PLT as low as 10,000 with ALL, so probably applicable to adults (JAMA 284(17):2222, November 1, 2000)
CT Findings with which LP Contraindicated
- Lateral shift of midline structures
- Loss of suprachiasmatic and basilar cisterns
- Obliteration of the fourth ventricle, or obliteration of the superior cerebellar and quadrigeminal plate cisterns with sparing of the ambient cistern
(Arch Intern Med 159:2681 December 13/27, 1999)
Reduction of Post-Dural Headache
Rational Clinical Exam Review (JAMA 2006;296:2012)
reinsertion of stylet was important
CSF-Blood glucose of 0.4 or less
CSF WBC of 500/uL or higher
CSF lactate level >3.5 mmol/L
accurately dx bacterial meningitis
bed rest not helpful
Para-median Approach
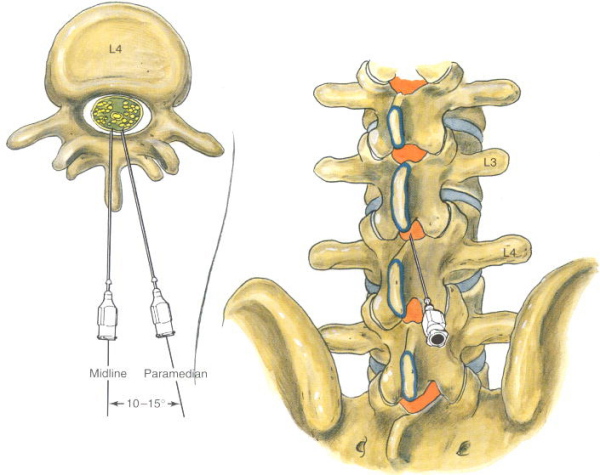
1 cm down and 1cm over from upper spinous process go 45 and 45 degrees
Leg Positioning
Acad Emerg Med. 2001 Jan;8(1):8-12.
no effect (~1 cm difference)
From Michelle Lin
When to Skip Head CT Before LP for Meningitis
Hasbun et al. CT of head before LP in adults with suspected meningitis.
NEJM. 345(24), 12/13/01: 1727-33
Design: Prospective observational single-site study (n=301)
Observed Results:
Got a CT (235/301)
–> 56/235 (24%) had abnormal CT
–> 11/56 had mass effect
High risk clinical features associated with abnormal CT:
· Age >= 60 yr
· Immunocompromised (HIV, transplant, immunosuppressive tx)
· History of CNS disease (mass lesion, CVA, focal infection)
· Seizure < 1 wk PTA
· ALOC
· Unable to answer 2 questions correctly
· Unable to follow 2 commands correctly
· Gaze palsy
· Abnormal visual fields
· Facial palsy
· Arm or leg drift
· Abnormal language / speech
Applying the high risk criteria back to the enrollment group:
Got a CT (235/301)
–> 96/235 had no high risk features (41%)
–> 93/96 (97%) had normal CT
–> 3/96 (3%) had 2 non-herniations and 1 mild herniation on CT
–> All 3 patients got LP without complications.
Results tracking saved time:
Time to antibiotics (3.8 hr for CT+ vs 2.9 hr for CT-)
Time to LP (5.3 hr for CT+ vs 3.0 hr for CT-)
Limitations:
* Study requires validation on separate population (diff from derivation group)
* Does NOT apply to r/o subarachnoid hemorrhage
Traumatic Taps
BMJ. 2015 Feb 18;350:h568. CONCLUSION: No xanthochromia and red blood cell count <2000×10(6)/L reasonably excludes the diagnosis of aneurysmal subarachnoid hemorrhage. Most patients with acute headache who meet this cut off will need no further investigations and aneurysmal subarachnoid hemorrhage can be excluded as a cause of their headache.