Small Bowel Obstruction
from the Mayo Clinic Blog:
The truth about Small Bowel Obstruction
Author: David S. Morris, M.D.
Small bowel obstruction (SBO) is a very common problem for patients; treated by many different types of medical providers, including primary care, emergency medicine, internal medicine, and surgery. In the United States alone, there are an estimated 300,000 laparotomies performed annually for SBO, and about one third of these obstructions are complicated by intestinal ischemia, with significantly higher morbidity and mortality resulting.
So every patient who shows up with a bowel obstruction should have surgery, to prevent ischemic complications, right? Actually, more than half of patients who present with SBO resolve with nonoperative therapy. Because the most common cause of SBO is post-operative adhesions, and each subsequent exploration carries a higher risk of unintentional damage to the intestine, surgical exploration therefore should be reserved for patients who absolutely need it.
So who needs an operation? Does it take years of surgical experience to know? What goes into the decision? First off, the traditional terminology used to classify bowel obstruction probably should be discussed. And then thrown out the window. Let me explain. During the past century or so, bowel obstructions have been dogmatically categorized as either partial or complete. But what does this mean, exactly? Partial bowel obstruction describes a patient who has dilated bowel on imaging, has nausea and vomiting, but continues to pass flatus or even stool intermittently. A complete obstruction has all the same signs and symptoms except for passage of flatus or stool. So the difference basically boils down to obstipation.
Now for the throwing out the window. Obstipation, which has been arbitrarily defined as no flatus or stool for more than 24 hours, is a very imprecise concept. When does the clock start on the 24 hours? And who really knows with absolute certainty when the last time flatus was passed (personally, I certainly don’t keep track that closely, do you). And if a patient has an obstruction associated with ischemia, why does it matter whether there is anything passing out the rectum?
A more useful way of thinking of SBO is operative vs. nonoperative. In the operative category, I would place the obstructions that are strangulated (by adhesions, hernia, or volvulus) as well as those that will not resolve with nonoperative therapy. Nonoperative obstructions are not strangulated, and will resolve without surgery.
Let me say a quick word about the pathophysiology of bowel ischemia in the setting of bowel obstruction. On a very basic level, and obstruction that results in, or is caused by, twisting of the mesenteric vasculature (volvulus, internal hernia, or adhesion-related mesenteric restriction) can, and often does, result in ischemic bowel. Patients with these types of problems are not difficult to identify clinically in most cases; these are the patients that present with excruciating pain, peritonitis, and possibly septic shock if perforation has already occurred. Diagnostically, they are the simplest patients – they need an operation or they will die.
Ischemia may also develop in a more insidious way. As an obstruction progresses, the bowel proximal to the point of obstruction becomes progressively more dilated over time as the succus and GI secretions accumulate. Healthy bowel can tolerate an impressive amount of dilation provided that such dilation occurs gradually. If the bowel is not healthy (history of IBD, prior surgery, radiation, etc.), or if the dilation happens quickly, the luminal pressures exceed the perfusion pressure of the intestinal capillary network, and blood flow stops. If effective decompression (either with surgery or with NG tube) does not occur promptly (typically around 6 hours or so), the ischemia may be irreversible, and the chance of intestinal perforation increases dramatically.
This latter type of bowel ischemia is the reason behind the traditional dictum in surgical training to “Never let the sun rise or set on a complete bowel obstruction.” If you wait too long, bad things can happen. But how reliably can a surgeon categorize bowel obstructions as complete or partial? It turns out, not very reliably, even when the surgeon has many years of experience. In one study, more than 50% of bowel obstructions with ischemia were misdiagnosed. Ouch!. An experienced surgeon is worse than a coin flip. That hurts on a deep level.
Fortunately, recent work done by my colleagues here at Mayo has improved our ability to identify ischemic obstructions. Dr. Martin Zielinski led a group of providers to create and prospectively validate a model to predict ischemic bowel obstruction. The team showed that three signs are associated with an ischemic obstruction: obstipation (no flatus or stool for 24 hours), mesenteric edema on CT scan, and absence of small bowel feces sign on CT.

Mesenteric edema (arrow) and small bowel feces sign (*)
If you don’t look at a lot of CT scans, you might be asking yourself, “What in the world is ‘small bowel feces sign?’” Well, trust me when I tell you that the appearance of the stuff in that loop of dilated bowel on that image looks exactly like the stuff inside the colon (i.e. poop), which you can see on the patient’s right side in the image above. Small bowel feces sign results from gradual trapping of fibrous material while allowing fluid to pass and be reabsorbed, and thus represents a more chronic process.
If a patient does not have any of the three Zielinski signs of ischemic obstruction, he or she might have a chance of resolving without surgery. Great! Problem solved! Admit them to the floor with an NG tube and IV fluids, and high fives all around, right?
The problem now becomes differentiating the patients who will resolve with nonoperative therapy from those who won’t. In many hospitals there are lots of patients sitting around in therapeutic limbo as the team takes a “wait and see” approach. Usually, after a few days or sometimes many days (this number is highly variable, depending on the surgeon, the patient, the day of the week, if it’s a holiday, the phases of the moon, etc. etc.), the patient is either getting better or is declared a failure of nonoperative therapy and gets a laparotomy. Studies seem to indicate that if the patient doesn’t resolve in less than three days, he or she probably needs an operation.
Is this the best modern medicine can do? Guess what — There is a better way. At the suggestion of a surgical resident, we investigated the use of soluble enteric contrast as a diagnostic adjunct in the management of small bowel obstruction. The “Gastrograffin® (GG) Challenge” became our standard of care for the patients who did not have ischemic SBO. Our protocol is as follows:
- Rule out ischemic obstruction (see “Zielinski signs” above)
- NG suction for at least 2 hours
- 100 ml of GG mixed in 50 ml of water and flushed down the NG tube.
- NG clamping x 8 hours
- Abdominal X ray at 8 hours.
If contrast is seen in the colon on X-ray, or if the patient passes flatus or stool while the NG is clamped, this is a “pass” and the NG is removed and diet is advanced. Hospital discharge typically happens sometime in the subsequent 24 hours. If no contrast is seen in the colon, or the patient does not tolerate 8 hours of NG clamping, or has recurrent nausea and vomiting with diet advancement, this is a “fail” and the patient gets an operation. We have had great success using this protocol, and have seen our length of stay improve significantly, because one way or another, the team knows which direction the patient is headed in only a few hours.
Let me finish with a few pearls for the non-surgeon, since I realize that most of the readers here are not my knife-wielding colleagues.
- If you think the patient has a bowel obstruction, go ahead and place a nasogastric tube. Placing a tube won’t make the patients like you, but by letting them stay bloated, and vomiting, and letting the ischemic cascade continue by not decompressing the bowel, you’re not doing the patients any favors. And don’t place the small-bore, soft silastic NG tube. They don’t work. The stuff that needs to come out is thick and nasty – like pond scum, in most cases – the small tube just will not do the job. The only thing worse than placing a large, stiff, NG tube is explaining to the patient that the soft “nice” tube that was placed initially is ineffective and that a large stiff tube is needed anyway.
- Patients with SBO can sequester liters and liters of fluid in the lumen of the bowel. Start some isotonic fluids. Run them in surgical doses, even for the dialysis patients and the heart failure patients. Intravascular depletion leads to poor perfusion, leads to bowel ischemia. We can deal with excess fluid when the obstruction is resolved.
- Make the patient NPO. Strict NPO. I’ve had patients drink gallons of ice chips while sitting in the ED. I’ve seen consults on the medicine floor where a patient is eating a cheeseburger around the NG tube. Remember the pond scum. Don’t add to it.
- Get a surgical opinion early on. My own (admittedly arrogant, heavily-biased) opinion is that SBO is a surgical disease, and should be managed by surgeons, even when operative therapy isn’t needed (cue the onslaught of hate mail, car bombs, and snarky comments from my surgical colleagues who disagree).
Further Reading
- Khasawneh MA, Ugarte ML, Srvantstian B, Dozois EJ, Bannon MP,Zielinski MD. Role of gastrografin challenge in early postoperative small bowel obstruction. J Gastrointest Surg. 2014 Feb; 18(2):363-8. Epub 2013 Oct 29.
- Zielinski MD, Eiken PW, Heller SF, Lohse CM, Huebner M, Sarr MG, Bannon MP. Prospective, observational validation of a multivariate small-bowel obstruction model to predict the need for operative intervention. J Am Coll Surg. 2011 Jun; 212(6):1068-76. Epub 2011 Mar 31.
- Bickell NA, Federman AD, Aufses AH Jr. Influence of time on risk of bowel resection in complete small bowel obstruction. J Am Coll Surg. 2005 Dec;201(6):847-54.
- Sarr MG, Bulkley GB, Zuidema GD. Preoperative recognition of intestinal strangulation obstruction. Prospective evaluation of diagnostic capability. Am J Surg. 1983 Jan;145(1):176-82.
Adhesions, herniation
Spasmodic pain in 3-5 min intervals
String of pearls, air fluid levels, step-laddering
NG tube, fluids, ABX
Never let the sun set or rise on a SBO
Obstructive Series
Need only Upright Chest and Upright Abdomen
A – Age over 50
B – Bowel sounds diminished
D – Distension (objective, not subjective)
O – Obstipation or constipation
X – previous surgery (a bit of a stretch – the “X” conjures up scars)
R – Ralfing (vomiting
)
Eur J Surg 1998 Oct; 164 (10): 778-84)
Also consider the elderly to evaluate for sigmoid volvulus
simple obstruction-bowel blocked, but vascular supply intact
strangulation-obstruction-vascular supply is compromised
closed loop-obstructed loop of bowel at both proximal and distal
partial vs. complete
the pain of strangulation is constant rather than colicky
drip and suck=conservative management
gastrograffin challenge
100 cc of gastrograffin is placed through the ng and then it is clamped for 2 hours
then get a simple abd film
Biondo S, Pares D, Mora L, Marti Rague J, Kreisler E, Jaurrieta E. Related Articles, Links Randomized clinical study of Gastrografin administration in patients with adhesive small bowel obstruction. Br J Surg. 2003 May;90(5):542-6.
Choi HK, Chu KW, Law WL. Related Articles, Links Therapeutic value of gastrografin in adhesive small bowel obstruction after unsuccessful conservative treatment: a prospective randomized trial. Ann Surg. 2002 Jul;236(1):1-6.
In the virgin abdomen
gastrograffin challenge and then CT scan
Intussusception
Small bowel volvulus in adults
Fluid filled small bowel twisted upon itself caused a closed loop and vascular compromise
Epidemiology:
· 5-10 times more common in third world than western world (Gurleyik)
· Responsible for 3%-6% of small bowel obstructions
· More common in pregnancy (volvulus responsible for ¼ SBO with SB volvulus first followed by cecal and sigmoid).
· 10 fold increase in Afghanistan during Ramadam
Etiology:
· Cause currently not completely understood
· High bulk diet eaten rapidly on an empty stomach
· May be secondary to abnormal mechanics (i.e. secondary to adhesions, Meckel’s diverticula, internal hernias, Ascariasis, or pregnancy).
Signs/Symptoms:
· Severe, central pain
· Signs of obstruction
Laboratory:
· Not helpful in making the diagnosis
Radiology: (Chou)
· Plain film radiographs: non-specific, may show only a gasless abdomen or signs of mild obstruction
· Barium swallow may show “corkscrew pattern”
· CT or MRI may show “”whirl” sign
· Angiography shows spiraling of the branches of the twisted SMA causing a “barber pole” appearance
Treatment:
· Immediate surgery with derotation and fixation or resection for ischemic bowel
Prognosis
· Mortality 10%-35%, much higher when bowel becomes ischemic
Inguinal Hernia
Incarceration” meaning to imprison or confine.[
refers to a hernia that is not reducible and without signs of obstruction or strangulation.
Obstructing hernias present with
signs and symptoms of an intestinal obstruction: nausea, vomiting, abdominal distension, obstipation, and abdominal pain. On examination, a prominent hernia might be apparent but can be difficult to detect in the obese patient or if the hernia is femoral in nature. Treatment is urgent and whereas some surgeons might attempt initial reduction and subsequent early elective repair, most would agree on early surgical intervention. Any attempt at manual reduction of an obstructed hernia should be performed under adequate sedation and analgesia and without excessive force to prevent intestinal perforation. Useful adjuncts to this include retraction of the testis to “break the suction force” and gently massaging the hernia toward the internal ring.
Strangulation implies a compromised vascular supply with gangrenous bowel and is a surgical emergency requiring immediate surgical attention. Patients with strangulation usually present with a hernia that is not only irreducible, but also shows signs of inflammation with redness, pain, and extreme tenderness. They can also have signs of intestinal obstruction and dehydration, progressing to sepsis and toxicity.
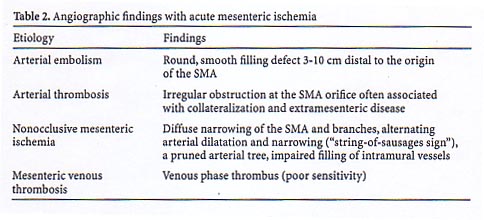
Mesenteric Ischemia
Most often in the SMA. Embolus or in 15-25% of cases thrombus (may have longer pain duration due to time to develop collateral circulation.)
A-Fib, CHF, dysrhythmias, MI predispose
Can also occur as a result of mesenteric vasospasm (Nonocclusive MI) in low flow states.
Severe colicky periumbilical abd pain c recurrent forceful BMs/Pain out of proportion to exam.
N/V. GI Bleed.
bowel empties as it gets more ischemic, so these patients WILL have diarrhea
Intestinal ischemia gives Ý phosphate, necrosis gives lactate
Superior Mesenteric Venous Thrombosis
accounts for ~5% of mesenteric Ischemia. Pain can progress over days to a week before presentation. Seen primarily in hypercoaguable states.
Intestinal Angina
chronic mesenteric Ischemia periumbilical pain 30 minutes after eating that lasts 1-2 hrs.
mesenteric venous thrombosis
ct shows hypodensity in trunk of SMV
associated with intraperitoneal fluid
and thickened segment of small bowel
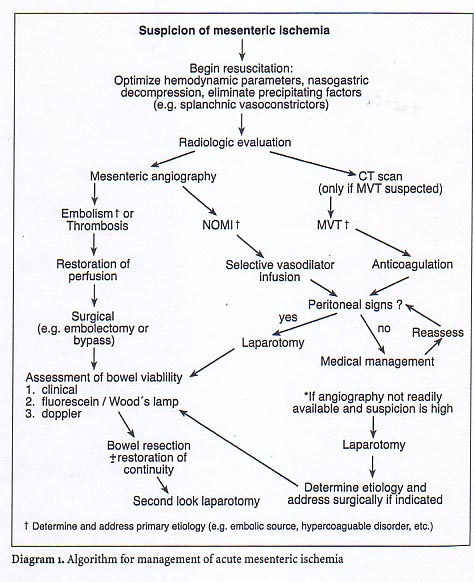
mesenteric ischemia arterial embolism (50%) arterial thrombosis (25%) nonocclusive mesenteric ischemia (NOMI) 20% mesenteric venous thrombosis (MVT) <5% start with plain abd film look for bowel wall thickening, thumb-printing, pneumatosis intestinalis, and portal vein gas NOMI-angiographically placed catheter infusion of vasodilators such as papaverine MVT gets heparin and possibly lysis or thrombectomy assessment of bowel viability is better with fluoroscein than judgement in arterial embolism/thrombosis
Small Bowel Ischemia Leukocytosis: common, nonspecific Hemoconcentration, metabolic acidosis with base deficit, hyperamylasemia: nonspecific, present in >50% Lactate: ~100% sensitive, 42 87% specific Ruotolo RA, et al. Clin Geriatr Med. 1999 Aug;15(3):527-57.
Differential Diagnosis:
· AAA
· Cardiac ischemia
· Mesenteric ischemia
The treating physicians were worried about the 3 vascular abdominal emergencies in the elderly and took steps to rule them out. Additionally, 22-40% of elderly ED patients with abdominal pain require surgical treatment and 7% of those >80 years will die.
Given the unchanged EKG and stable vital signs a stat abdominal CT was ordered along with immediate surgical consult for possible mesenteric ischemia. Final radiologist reading of a triple contrast CT was: Intrahepatic biliary dilatation and small amount of perihepatic fluid consistent with acute hepatic process and large amount of colonic stool consistent with fecal impaction.

Diagnosis?
Can this patient be discharged with the diagnosis of constipation and/or “an acute hepatic process”?
Thankfully the initial reading of the CT by the radiology resident was: distended small bowel with a thickened wall, some free fluid, and mild biliary dilatation.
Although the CT scan was consistent with mesenteric ischemia, the patient’s pain improved intermittently after Fentanyl and the surgical service declined to operate immediately on the patient. The new shift of emergency physicians ordered a mesenteric angiogram, which was done approximately 2 hours after being ordered. Initial reading of the angiogram was consistent with mesenteric ischemia.
Acute Arterial Occlusive Mesenteric Ischemia
Pathophysiology:
· Thrombosis or emboli occlude arterial blood supply to intestines
· Emboli almost always involve the superior mesenteric artery
Epidemiology:
· Occurs almost exclusively in patients with atherosclerotic disease
Etiology:
· Emboli most often from clot in the left atrium or ventricle, occasionally from aortic thrombus
· Thrombus develops via atherogenic process
· Cardiac and/or vascular pathology common: CAD, valvular disease, atrial fibrillation, post MI mural thrombi, aortic instrumentation
Signs/Symptoms:
· Sudden onset of severe periumbilical pain
· May have nausea, vomiting, and diarrhea
· Hallmark: pain out of proportion to physical exam
· 75% of patient have heme negative stool
· If ischemia progresses untreated, the patient will develop tenderness, peritoneal signs, and shock
Laboratory:
· No test sensitive enough to rule out diagnosis reliably
· Lactate, WBC, and phosphate studies: only elevated consistently when bowel is already necrotic; Leo found phosphate only 26% sensitive.
· Labs may be entirely normal early on in course of disease
Radiology:
· Plain films
1) Usually normal or nonspecific
2) Late findings include intramural air (pneumatosis intestinalis), thickened bowel wall with “thumbprinting”, and portal venous gas
· CT Scan
1) Often normal or non-specific
2) Most common finding: bowel wall thickening (non-specific)
3) Specific findings include pneumatosis intestinalis, portal venous gas, abnormal bowel enhancement, and mesenteric vessel occlusion
4) Sensitivity 64%-82% (Taourel 1996) but can diagnose other important pathologies in the differential.
· Doppler ultrasound and MRI not well studied, may be helpful in the future
· Angiography
1) Gold standard
2) Only for stable patients without peritoneal signs; patients with an acute surgical abdomen should go directly to surgery
Treatment
· Aggressive diagnostic approach warranted as mortality is significantly increased by small delays in treatment.
· Most patients require fluid resuscitation secondary to third space fluid loss.
· Surgical resection of ischemic bowel and/or embolectomy of involved vessel have been the standard of care.
· Newer therapies involve intra-arterial infusions of papaverine or thrombolitics coupled with laparoscopy in patients without peritonitis. ( Regan 1996)
Hospital course:
The patient was taken to the operating room with a pre-op diagnosis of mesenteric ischemia. In the OR, surgeons found that in the middle portion of the jejunum, the small bowel was twisted to the point that it became strangulated. Final reading of the angiogram showed: Non-opacification of the distal jejunal branches, ileal branches and ileocolic branch of the superior mesenteric artery. No definite evidence of embolism is identified. Moderately dilated bowel in the region of hypovascularity. These findings are suggestive of a mid gut volvulus.
True diagnosis: intestinal ischemia secondary to small bowel volvulus
Teaching points:
1) Suspect mesenteric ischemia in all elderly with severe abdominal pain without significant tenderness.
2) Don’t be dissuaded from a proper diagnostic evaluation by radiographic diagnoses that don’t fit the severity of the patient and when faced with 2 interpretations always consider the most dangerous one first.
3) The only methods to “rule out” mesenteric ischemia are angiography and surgery, but CT often will provide alternative important diagnoses.
Hepatic Portal Venous Gas On CT Scan in the ED Hepatic portal venous gas (HPVG) is a radiologic finding that occurs when gas from the intestinal lumen passes through the intestinal wall and travels via the mesenteric veins to the portal vein and into the liver. Most cases of HPVG are related to mesenteric ischemia and this finding has traditionally been associated with a high mortality. However, CT scan has greatly increased the sensitivity for the detection of HPVG. As a result, the clinical outcome of patients with mesenteric ischemia has improved and there has been an increasing rate of detection of HPVG with certain nonischemic conditions. Conditions that have been reported to result in HPVG include inflammatory bowel disease (both CrohnÂs disease and ulcerative colitis), diverticulitis, intestinal obstruction, blunt abdominal trauma, gastric ulcer, intraabdominal abscess, cholangitis, and complications of iatrogenic procedures (e.g. ERCP and colonoscopy) (1-4). Emergency Physicians, then, need to be aware that HPVG is not a specific disease entity, but merely a diagnostic clue in patients with acute abdominal pathology and when portal venous gas is detected in the ED, it is important to differentiate life-threatening mesenteric ischemia from other more benign nonischemic causes (1). It is known that the presence of HPVG carries a much less severe prognosis when found on CT as compared to the finding of gas on plain radiographs (1,4). Therefore, the finding of HPVG on CT should be carefully evaluated in the context of clinical findings. In certain cases, the prognosis is favorable and surgery is not required. However, when CT demonstrates portomesenteric vein gas and clinical findings suggest the presence of mesenteric ischemia, surgery is mandatory. Of note, it has been reported that the presence of gas simultaneously in the portal venous system and intestinal wall seems to be specific to intestinal ischemia (5).
| | |