Urinary Tract Infections
Diagnosis
Dipstick 78-92% sensitive and 65-96% specific
Metaanalysis showed Sensitivity of 75% for the dipstick (Emerg Med J 20:362, 2003)
1. Escherichia coli
2. Staphylococcus aureus*
3. Klebsiella pneumoniae
4. Proteus mirabilis
5. Enterococcus* faecalis
6. Pseudomonas aeruginosa
7. Enterobacter cloacae
8. Citrobacter
§ = Listed in order of decreasing frequency * = Gram-positive organisms
Corynebacterium, Lactobacillus, and Streptococcus species are identified only rarely; when they are present, they nearly always represent contamination of the specimen rather than a true pathogen. In complicated UTI, in addition to E. coli, there is a higher prevalence of Pseudomonas, Enterobacter species, Serratia, Acinetobacter, Klebsiella, and enterococci.
Rx
Uncomplicated UTI: ½ Dose Fluoroquinolone for 3 days or consider 1st gen. cephalosporin, nitrofurantoin for a week. Agent of choice at this point should be Cipro XR 500 mg OD or Cipro 250 BID. 3 days in uncomplicated UTI is sufficient.
Give phenazopyridine 100-200 mg TID for no more than 48 hours.
Complicated UTIs:
Underlying abnormality
Immunocomprimised Host
Urinary Tract Obstruction
Failed Out-Pt management
Progression of uncomplicated UTI
Persistent Vomiting
Renal Failure
Urosepsis
Age>60
No follow-up or poor social situation.
Treat for 10-14 days
Pyelo (Outpt): Full Dose Fluro for 1 week or 1st Gen Ceph for 1 week
fosfomycin tromethamine 3 g, single oral dose. The single dose is well-absorbed, produces therapeutic concentrations in urine for 2-4 days, The suprapubic discomfort or dysuria common with UTI can be treated with phenazopyridine (adults, 100 mg 2 tablets tid or 200 mg 1 tablet tid not to exceed two days of therapy; children ages 6-12, 12 mg/kg/d divided into tid dosing not to exceed two days of therapy).11 Elderly females with lower tract UTI symptoms and no systemic complications may be treated for three days with regimens similar to those prescribed for younger women
Pyelo (Inpt):
Ciprofloxacin 400 mg IV bid
Alternative:
Gatifloxacin 400 mg IV qd
Levofloxacin 250 mg IV qd
Ofloxacin 400 mg IV bid
Ampicillin 150-200 mg/kg/day divided q 3-4 h (gentamicin 5-7 mg/kg qd)
Cefotaxime 1-2 g q 4-12 h
Ceftriaxone 1-2 g IV qd
Complicated Pyelo (Inpt):
Ciprofloxacin 400 mg IV q 8 hr + (tobramycin 5-7 mg/kg/day)
Ampicillin 150-200 mg/kg/day IV divided q 4 h (tobramycin)
Pipercillin/tazobactam 3.4 g IV q 6 or 4.5 g q 8
Ticarcillin/clavulinic acid 3.1 g IV q 6
Imipenim 0.5 g IV q 6
Blood cultures in immunocompetent patients appear to have little value (Annals Emerg Med 2005;46(3):285)
UTI in Women
obstruction, instrumentation. E Coli and Staph
Upper Vs. Lower Tract
1 day, 3 day, 7-10 day of Bactrim
Cipro 250 bid or keflex (can also be used for mild pyelo) Upper tract gets 2 weeks
Always Rx pregnant women: nitrofurantoin or keflex
for sx relief-pyridium 200 mg pot id (max 2 days)
Suprapubic Puncture for kids <1 yr
Hemorrhagic cystitis
If recurrent uti, consider paraurethral gland infection from chlamydia, give doxy for 2-4 weeks
Clean catch is fairly useless (Arch Intern Med 160, 200)
UTI in men
Urethritis-Gonococcal and non. Ceftriaxone 250 mg IM and Doxy 100 BID x 1 week
Prostatitis-1 month of Rx
Epididymitis (usually chlamydia)-treat as for STD
Orchitis-can be viral (mumps) or bacterial
antibiotics (trimeth) reduces duration of sx even if dip negative (BMJ 2005;331;143) Dee Richards, Les Toop, Stephen Chambers and Lynn Fletcher blind randomised controlled trial negative dipstick urine test results: double symptoms of urinary tract infection but Response
UA Stuff
Specific Gravity
SG 1.002 correlates with osmal of 50-100
SG 1.030-1.040 correlates with osmal 1000-1200
1.010 is is isosthenia; correlates with osmal (300). Indicative of renal tubule damage
Glucose makes urine look more concentrated than it is; IV contrast does the same
Urine pH
normally acidic (4.5-6.5)
if urine pH is high, suspect a UTI: proteus cleaves urea into NH4
Glucose
Ketones
Urine dipstick measures acetone and acetoacetate
Billirubin
conjugated billi is water soluble and excreted in urine when elevated
Nitrites
nitrates are normally present in the urine. Gram negatives reduce nitrates to trites.
Leuk Esterase
neutrophil specific esterase; indicates presence of WBCs. Any inflammatory cause
Protein
Specificity of the urine nitrite test for urinary tract infection decreases as a function of increasing serum bilirubin. Most patients with hyperbilirubinemia and a positive nitrite test in our sample did not have an associated urinary tract infection. (The American Journal of Emergency Medicine Volume 25, Issue 1 , January 2007, Pages 10-14)
URINE DIPSTICKS
A report in Evidence Based Medicine summarises research into the value of dipstick results in women suspected of having urinary tract infection. Urine dipstick testing was found to be of relatively limited value, with negative test results failing to satisfactorily rule out infection. (Evid Based Med 2009; 14: 155)
Nephrolithiasis
In pts with CT Scan + for stone
Dipstick:
sensitivity, specificity and diagnostic accuracy were 80%, 35% and 57%, respectively.
UA c 1 RBC considered Positive 89%, 29% and 58%
UA c >1 RBC Considered Positive 81%, 49% and 65%
UA c >5 RBC Considered Positive 67%, 66% and 67%
(J Urol 162:685, September 1999)
UA was at least trace positive for blood in 84% of the patients with ureterolithiasis and in 52% of patients with completely negative CT scans or scans demonstrating alternate diagnoses. At this RBC threshold hematuria on microscopic urinalysis had a sensitivity and specificity for ureterolithiasis of 84% and 48%, respectively, and positive and negative predictive values of 72% and 65 respectively. If a cut-off of 10 RBC/ml or higher is used as an indicator of hematuria, the sensitivity and specificity of hematuria as a marker of renal colic were 81% and 51 respectively, and the positive and negative predictive values were 73% and 62%, respectively. The urinalysis was falsely negative in 17% of patients with ureteral stones measuring 5mm or less, and 11 of those with larger stones. (Urology 59(6):839, June 2002)
The American Journal of Emergency Medicine Volume 21, Issue 6 , October 2003, Pages 492-493
The purpose of this study was to determine whether the presence of hematuria or its absence can predict the presence or absence of urinary calculi as determined by computed tomography (CT) scan in patients presenting to the ED with acute abdominal colic. We reviewed the urine analysis and CT scans of all patients presenting to the ED over a 12-month period with acute colic and a clinical suspicion of urinary calculi. Urine samples were drawn on arrival in the ED before CT scanning. Two hundred seventy-seven patients were included in the study. The prevalence of urinary stones as detected by CT was 57.4%. The positive predictive value, negative predictive value, and accuracy for hematuria as a marker for stone disease was 60.9%, 72.4%, and 62.1%, respectively. A total of 3.24% of patients had some degree of obstruction, all of whom had hematuria. The absence of hematuria is not a reliable exclusion criterion for urinary calculi. The detection of urinary stones without hematuria does not imply obstruction.
The authors suggest that about 95% of ureteral stones measuring 4mm or less will pass spontaneously, but passage may require up to 40 days, and that about half of patients with larger stones may require a stone recovery intervention (J Urol 162:688, September 1999)
Crohn’s patients are prone to stones secondary to hyperoxaluria, Elevated pH points to stuvite stone.
Infected Stones
UTI with obstructing stone is an emergency. UTI coincident with stone is not
“Association of Pyuria and Clinical Characteristics With the Presence of Urinary Tract Infection Among Patients With Acute Nephrolithiasis”
http://www.ncbi.nlm.nih.gov/pubmed/23850311
fever & >5 wbc on 86% sensitive and 79% specific for UTI
NHCT is more accurate than IVP (Annals EM 40, 2002; p. 280)
The flat plate radiograph uses the same orientation and anatomical presentation that is observed on fluoroscopy, retrograde pyelograms, or during endoscopic ureteral surgery, such as ureteroscopy or intracorporeal lithotripsy. Even if a stone is not visible on a flat plate radiograph, the calculus could be a radiolucent uric acid stone that can be dissolved with alkalinizing medication. Such a stone is more likely if the urine pH indicates very acidic urine. In practice, any patient with symptoms of acute renal colic who demonstrates a urine pH lower than 6.0 should be considered at risk for a possible uric acid stone and should have a KUB radiograph performed to help determine radiolucency. The flat plate radiograph is inexpensive, quick, and usually helpful even if no specific stone is observed. It is extremely useful in following the progress of previously documented radiopaque calculi and checking the position of any indwelling double-J stents. The KUB radiograph can suggest the fluoroscopic appearance of a stone, which determines whether it can be targeted with extracorporeal shock-wave lithotripsy (ESWL). The KUB radiograph is also quite accurate in determining the exact size and shape of a visible radiopaque stone, which can only be estimated using a CT scan alone because the x-ray beam of the CT scan does not always cross the stone at its widest point. Differentiation between a phlebolith and an obstructing calcific stone becomes easier when the KUB radiograph demonstrates a lucent center, identifying the calcification as a phlebolith. This central lucency is not observed as often on CT scanning. Many urologists recommend the flat plate radiograph in addition to CT scan for any renal colictype scenario for these reasons. A number of studies have suggested that the flat plate has a relatively low sensitivity and specificity for renal and ureteral calculi. Many patients have numerous pelvic calcifications that make pinpointing specific stones difficult. Any calcific density observed on KUB radiograph that happens to overlie the course of the ureter is not guaranteed to be a stone. A number of emergency physicians argue that the flat plate radiograph adds little to the identification and treatment of a stone in the ED. Furthermore, obtaining a flat plate radiograph may cause delays, may unnecessarily increase the cost of the workup, and produces additional patient radiation exposure; consequently, flat plate radiograph is no longer required in the modern era when unenhanced CT scans are now the criterion standard for diagnosis of acute renal colic. A large clinical study from Johns Hopkins by Jackman and associates (2000) concluded that “plain abdominal x-ray is more sensitive than scout CT for detecting radiopaque nephrolithiasis. Of the stones visible on plain abdominal x-ray, 51% were not seen on CT. To facilitate outpatient clinic follow-up of patients with calculi, plain abdominal x-rays should be performed.” Many urologists, including this author, recommend that a KUB radiograph, in addition to other studies such as noncontrast helical or spiral CT scans, be obtained in patients with a clinical presentation of acute flank pain suggestive of renal colic. Knowing the exact size and shape of a stone, its position, fluoroscopic appearance, surgical orientation, and relative radiolucency is an advantage. Also, the progress of the stone can easily be monitored with follow-up flat plate radiograph. These advantages far outweigh the few disadvantages of performing the examination. The digital CT scout radiograph can be used as a reasonable substitute for the KUB radiograph if cost factors, excessive delays, or logistical problems make obtaining a formal abdominal flat plate study difficult. (Emedicine)
Pain Meds
Morphine plus ketorolac is better than either of them alone (Ann Emerg Med 2006;48:173)
Alpha Blockers
Use flomax o.4 mg po qd until uro f/u
The comparison and efficacy of 3 different alpha1-adrenergic blockers for distal ureteral stones. (J Urol. 2005 Jun;173(6):2010-2) Randomized trial of the efficacy of tamsulosin (flomax), nifedipine and phloroglucinol in medical expulsive therapy for distal ureteral calculi. (J Urol. 2005 Jul;174(1):167-72)
Lancet. 2006 Sep 30;368(9542):1171-9. Although a high-quality randomised trial is necessary to confirm its efficacy, our findings suggest that medical therapy is an option for facilitation of urinary-stone passage for patients amenable to conservative management, potentially obviating the need for surgery. SR (Ann emerg med 2007;50:552)
RCT which was underpowered and had no real size stones showed no benefit (Ann Emerg Med 2009;54:432) pH>7.6 consider proteus or morganella morganii no damage to kidney with obstruction for 2-4 weeks Urolithiasis was present (as defined by low-dose unenhanced MDCT) in 507/638 patients (79%); 341/638 (53%) were true positive for urolithiasis, 76 (12%) were true negative, 55 (9%) were false positive and 166 (26%) were false negative. Microhaematuria as a test for urolithiasis in patients presenting to the emergency department therefore has a sensitivity, specificity, positive predictive value and negative predictive value of 67%, 58%, 86% and 31%, respectively. 58% of the urinalysis results were negative for haematuria in the subset of patients with significant alternative diagnoses. (Emergency Medicine Journal 2008;25:625-630)
Urinary Retention
Etiologies include: bph, prostate ca, urethral strictures, nephrolithiasis, bladder neoplasm, phimosis, meatal stenosis, post urethral valves (peds), ureterocele (women), prostatitis, cystitis, anticholinergic and sympathomimetic drugs, neurogenic lesions, post-operative,
There is no utility to gradual bladder drainage. Hematuria will happen anyway, decreased blood pressure is probably just BP returning to pre retention levels and risk of renal damage is higher with continued obstruction.
Men presenting with AUR caused by BPH were randomized to immediate removal, or removal at 3 or 7 days. Sixty-two percent of the men randomized to the 7-day catheter group were able to void successfully after removal of the catheter. Rates for men in whom the catheter was removed immediately or after 3 days were 44% and 51%, respectively. The authors of this study conclude that men with AUR who are found to retain volumes in excess of 1300 ml should have longer periods of catheter placement to increase their chances of subsequent successful voiding
(Emergency Medicine Clinics 19:3, August 2001 & Mayo Clin Proc 72:951, October 1997)
Fourniers Gangrene
Necrotizing fasciitis, from skin, urethra, or rectum
Associated c instrumentation, strictures, obstruction of urethra
Predisposing factors are dm, trauma, paraphimosis, uti
Get blood and wound cultures
Rx mixed flora and anaerobes
Crepitus, fever, swelling, tachy, temp
Get KUB and/or scrotal uts to look for free air
IVF, Unasyn or Ceft, Gent, Clinda
High Mortality
Foley Issues
Catheter removal can sometimes be difficult.
three possibilities:
(1) the valve where water is injected into the catheter may be blocked;
(2) external clamping or kinking may have damaged the tube; and
(3) crystallization of the fluid used to inflate the balloon may be preventing the balloon from deflating.
The first step is to cut the balloon port proximal to the inflation valve. If this does not result in a release of water, and ability to remove the catheter, then a wire is passed through the inflation channel. The wire from a central venous cannula set is appropriate for this task. The wire may be passed into the balloon and used to perforate it. However, sometimes a firmer structure is needed and, in this case, the venous catheter itself is used. It is passed over the guidewire into the balloon.
If the venous catheter does not rupture the balloon, leave the catheter in place and use it to introduce chemicals into the balloon. These chemicals will sufficiently degrade the balloon so that it ruptures but does not disintegrate. Chemicals such as ether, chloroform, acetone or mineral oil are used. Of these, mineral oil is recommended. Ten ml of mineral oil are drawn up into a syringe and introduced into the catheter balloon. After waiting for about 15 minutes, an attempt is made to remove the urinary catheter. If unsuccessful, an additional 10 ml is instilled.
If the balloon ruptures, inspect it carefully and ensure no bits have been left behind. They can act as a nidus for Infection, or calculus formation, and can produce significant irritation when voiding.
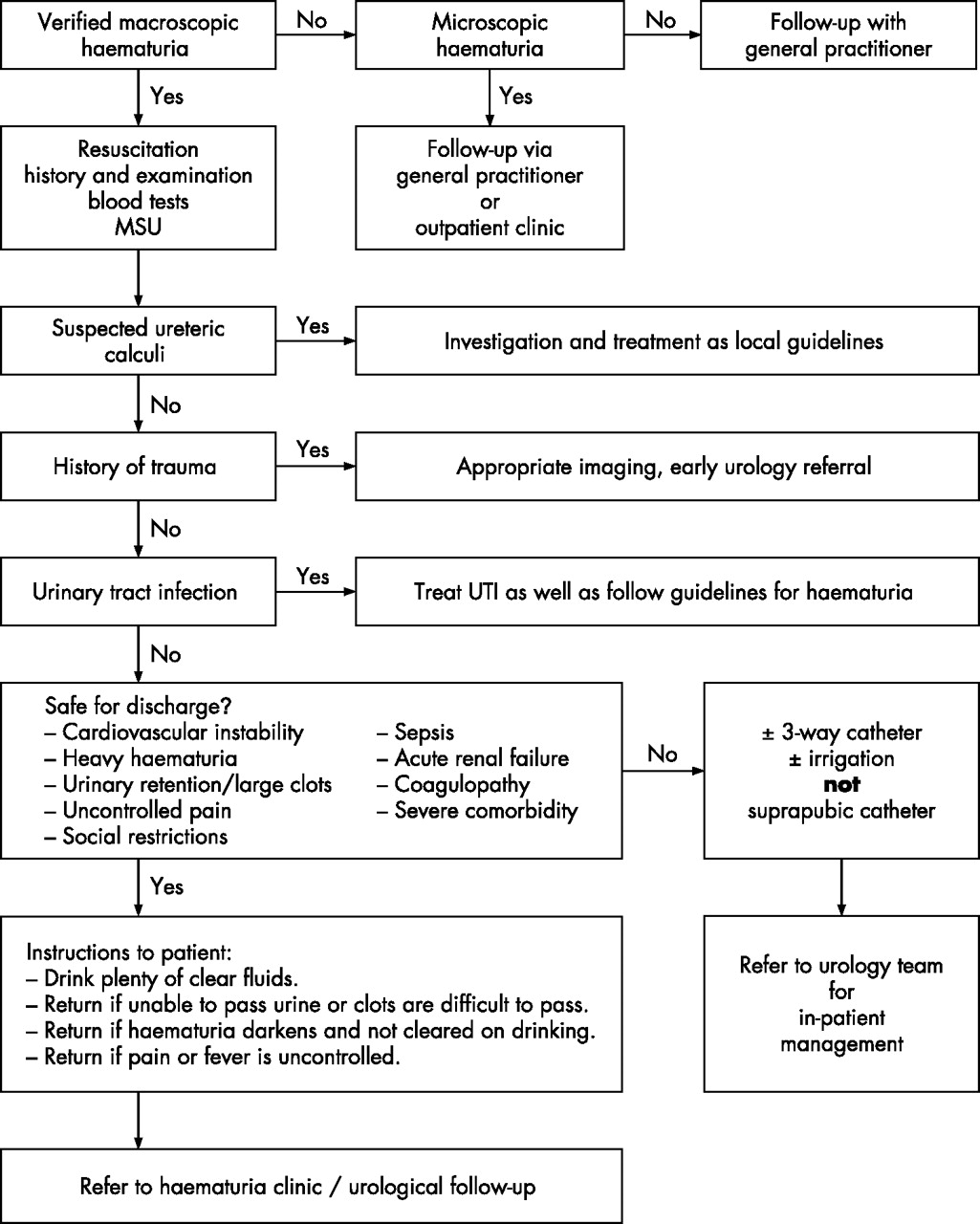
Macroscopic Hematuria
Box 1: Differential diagnoses in macroscopic haematuria
- Urinarytract malignancy: kidney, renal pelvis, ureter, bladder, prostate,urethra
- Urinary calculi
- Infections: urinary tract infection,schistosomiasis
- Trauma: penetrating or blunt
- Benign prostatichyperplasia
- Haemorrhagic cystitis
- Endometriosis
- Nephrologicaldisease: IgA nephropathy, glomerulonephritis
- Postproceduralbleedingfor example, transurethral surgery
- Bleedingdisorders, anticoagulation therapy above therapeutic range
- Arteriovenousmalformation/angiomyolipoma
(Emerg Med J 2007)
Male GU Problems
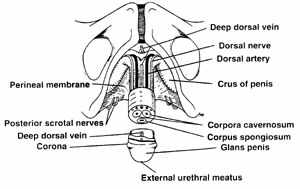
Penile Ring Block
infiltrate subcutaneous lidocaine (without epinephrine) circumferentially at the base of the penis
Balanitis And Balanoposthitis
Balanitis is an inflammation of the glans, while posthitis is an inflammation of the foreskin. Balanoposthitis refers to the presence of both conditions.
Rx: nonspecific c oral PCN and Fungal (candida) c antifungal cream
Testicular Torsion-Time is testicle.”
cremasteric reflex on each side, use a tongue blade. observe for more than 0.5 cm elevation of the ipsilateral testis. Of all physical exam findings, the presence of the cremasteric reflex appears to be one of the most helpful in ruling out torsion
96% negative predictive value for testicular torsion. Pediatr Surg Int 1999;15
Palpate the testicle and scrotal contents for localized tenderness and masses. Have the patient stand to note how the testicle lies in the scrotum. The normal testis rests in the vertical axis with the superior pole tipped slightly forward. The epididymis is located above the superior pole in the posterolateral position
“Prehns sign” has been found to be extremely unreliable and should not be usedeven patients with torsion can feel some relief of pain with this maneuver. The acute scrotum. Emerg Med Clin North Am 1988;6(3)
Torsion of a testicular appendage will often result in a palpable tender nodule in the testicle near the epididymis.
Radiologic Imaging: “Castration Through Procrastination?”
Any patient who presents with a classic case of testicular torsion should never see the inside of a radiologic suite.
Doppler ultrasound has replaced nuclear imaging in many institutions. Color-flow Doppler can detect decreased intratesticular blood flow. It is very sensitive for detecting increased blood flow associated with scrotal inflammation secondary to epididymitis or appendix torsion. However, the sensitivity for torsion ranges from 83%-100%. It appears to be accurate even in those patients who have equivocal clinical findings. Color-flow Doppler is less specific in small children and especially neonates as it cannot detect blood flow in a testis smaller than 1 mL volume. In neonates, up to 40% of normal testes will show no blood flow.53-55
Treatment And Prognosis Of Testicular Torsion
Once torsion is strongly suspected, either clinically or radiographically, call the urologistquickly. While awaiting his or her arrival, consider manual detorsion. There is no large study that demonstrates which is the best way to untwist the spermatic cord. Manual detorsion is successful in approximately 25% of patients, and counterclockwise twisting seems to be more common.
Successful manual detorsion does not preclude an urgent scrotal exploration, as retorsion may occur at any time.
Most studies report a high viability of the testis70%-100%if detorsion is achieved within 10 hours. Beyond 10 hours, the salvage rate drops to 20%. Urology 1978;11(1)., Torsion of the spermatic cord: a review of the literature and analysis of 70 new cases. J Urol 1970;104(4)
However, there have been reports of testicular salvage after several days of torsion, although the twisting was not as severe or may have been intermittent.
crude measure of testicular blood flow is done with a handheld Doppler probe (normally used to detect pulses). (See Figure 3.) Placing the probe over the normal testicle should allow detection of an arterial pulse. Compression of that testicles spermatic cord and artery should block the signal, and can be useful if questions on the source of the signal exist. The flow signal should be absent on the torsed side. Again, this is a crude measure, but if no pulse is detected, it may prompt more urgent urologic consultation. Reappearance of the flow signal and pain relief can be established as goals in manual detorsion.

Scotal Mass
Testicular Tumor
Urinary Retention-Can try coude cath (upward part points anterior) Suprapubic-2 finger breadths above symphysis, direct towards rectum.
Prostate exam, also check bulbocavernous reflex to evaluate sacral nerves.
Document full neuro exam to show you looked for compressive lesion/abcess causing neurological urinary retention
No problem emptying the entire bladder at once(Dan Med Bull 1984;31(1))
Trauma Induced Testicular Torsion: a Reminder for the Unwary
Trauma induced testicular torsion is a well recognized entity, the incidence being 4-8% in most series on testicular torsion (1). The signs and symptoms of torsion may easily be mistakenly attributed to preceding acute trauma. It may be very difficult at times in the ED to distinguish clinically between torsion and acute injury. Not uncommonly, the presentation is ascribed to a diagnosis of scrotal hematoma, only to have the patient return at a later date after testicular salvage is no longer possible. A high index of suspicion is required of the clinician to look past the injury and consider torsion as a possibility. “The message that trauma can and not infrequently does precipitate torsion needs to be reiterated” (1).
Nontraumatic hematuria
RBC Casts=kidney
Red urine can also be from beats or food coloring
Stones-calcium oxalate, Stuvite (Alkaline Urine, from proteus), Uric Acid (radiolucent), Cysteine (radiolucent). Pt will be writhing. Spiral CT or UTS
RTAs
Hypokalemia-ph<5.5-II, pH>5.5-I
Hyperkalemia-IV from decreased rennin/aldosterone-diabetes, ACEIs, HIV, adrenal disease)
Priapism
When examining the penis, palpate the glans to ascertain whether it is hard or soft.
Patients with low-flow priapism usually have a rigid, painful penile shaft with a soft glans.
This is because the corpora cavernosa are erect but the corpora spongiosum remains flaccid. Low-flow is a time dependant emergency.
However, all patients with priapism can be initially treated with terbutaline 0.25-0.5 mg subcutaneously in the deltoid muscle. The management of low-flow idiopathic priapism includes corporal blood aspiration, as previously described, followed by corporal injection of 200 mcg of phenylephrine (dilute 1 mg of phenylephrine in 9 mL sterile water to achieve a concentration of 1000 mcg/mL).Five to 10 cc of the lidocaine is deposited in a subcutaneous ring taking care to avoid intravascular injection. After this is completed, the physician stands to the right of the patient and grasps the penis with the left hand. Palpate the engorged corpora cavernosum bilaterally and, after preparing the skin with Betadine, insert a 21- to 19-gauge butterfly needle into either side at the 10 oclock or 2 oclock position. The needle may be placed anywhere from the base of the penis to the distal shaft, avoiding the glans. Avoid deep penetration to minimize risk of injury to the cavernosal artery. Aspirate 20-30 mL of blood while milking the corpus with the other hand. Continue aspiration until the egress of dark blood ceases and bright-red arterial blood is obtained.11 Low-flow priapism is suggested by aspirated blood with a pH of < 7.25, pO2 < 30 mmHg, and pCO2 > 60 mmHg.
If there is difficulty in differentiating low- vs. high-flow priapism, blood gas measurement from a cavernosal sample may help. Values similar to arterial blood are indicative of high-flow priapism, whereas samples more consistent with venous blood sampling suggest the low-flow etiology. Utilizing a blood gas needle and syringe, samples are drawn in similar fashion to corpora aspiration, which is described later in this article. Blood gas measurements of pH can give an indication of the urgency based on the degree of acidosis. A pH less than 7.10 reflects more aggressive management options should be sought quickly in that the tissue is at risk for necrosis Ice and elevation are also components of the initial conservative therapy. A penile dorsal nerve block utilizing local anesthesia may be of benefit to control pain. This requires raising a circumferential wheal of local anesthesia without epinephrine around the base of the penis at a site approximately one centimeter distal to the pubic bone and scrotal insertion.Terbutaline also can be given subcutaneously in doses of 0.250.5 mg and can be repeated in 1520 min Treatment with injections into the corpus cavernosum of alpha adrenergic receptor agonists after aspiration would be the next therapy after terbutaline. Phenylephrine, 10 cc, which corresponds to a dose of 200 ug (usually 1 mg diluted in 100 cc of saline), is injected into the penis after aspiration. See Table 2 and Table 3 for specifics of the aspiration and injection procedure and equipment required. Figure 2 demonstrates the injection of anesthesia locally into one of the corpora cavernosa, which would be the same angle as the butterfly needle used for aspiration. Failure to respond can be followed by a second injection of 200 ug and, if needed, a final dose of 500 ug. Frequent blood pressure monitoring is required throughout treatment. Alternatively, epinephrine (1.0 mg diluted in 100 cc saline) can be injected in 13 cc boluses up to 10 cc [13]. Pseudoephedrine 60100 mg also can be injected into the cavernosa.(JEM April 2004)


Best Blog Post
Epididymitis
If GC/Chlamydia can not treat with one dose therapies, give 2 weeks antibiotics
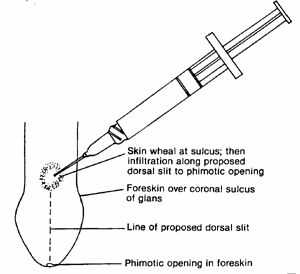
Phimosis
Cant withdraw the foreskin, Foley if can not pee through. Can place a dorsal slit.
Rx for infection-bacitracin or diflucan 200 mg po x1
Paraphimosis
Can not put foreskin back into place
May need to cut
Koro
| | |