Hemorrhagic Stroke-Spontaneous Intracerebral or Intracranial Hemorrhage
Best ReviewAnother Good Review
Hem Stroke review by Oli Flowers
AHA Guidelines for the management of spontaneous Intracerebral hemorrhage
(Stroke 2010;41)
Pertinent New Stuff:
Added may consider PCC, but no clinical benefit demonstrated over FFP (IIa;B)
Reversal of Anti-plt agents is considered investigational
Acute lowering of BP to SBP of 140 is probably safe (IIA;B)
Patients should be admitted to ICU (I;B)Avoid Hypoglycemia, tight glucose control not recommended (I;C)Prophylactic Anticonvulsants should not be used (B)Consider ICP monitoring if GCS <9, sig. IVH, hydrocephalus, or herniationMaintain CPP 50-70 and ICP < 20 (IIb;C)Intraventric admin of tpa for IVH is considered investigational (IIb;B)Cerebellar hemorrhage with poor mental status or hydrocephalus need surgery (I;B)Consier crani in patients with lobar clots > 30 ml within 1 cm of surface (IIb;B)Withhold making decision to withdraw agressive care until 2nd full hospital day (IIa;B)—Bleed location in hypertensive bleeds (in order of prevalence)Basal GangliaThalamusPonsCerebellarconsider angio in young patients or ones with vascular abnormalities, perisylvan bleeds, abnormal calcification BP MAP 70-130 (110 immediately post-op or in patients with no preexisting hypertension) seizure proph only if increased icp or seizure pts with GCS < or = to 4 without cerebellar compression are not recommended for surgery —————————————————- Early growth of hemorrhage and outcome (Stroke 1997;28:1-5) 1/4 of the hemorrhages grew substantially on 1 hr repeat CT it is often associated with neurologic deterioration ————————————————– ICH Grading Score (Stroke 2001;32:891) in previous studies only 1 in 35 of pts with GCS 3 or 4 survived to 30 days ———————————————————– European guidelines (Cerebrovasc Dis 2006;22:294) ———————————————————- Surgical vs conservative treatment for ICH: STICH (Lancet 2005;365:357) ——————————————————
Acta Neurochir (Wien). 1981;58(3-4):203-11. Links Sodium nitroprusside and intracranial pressure. The effects of sodium nitroprusside on intracranial pressure were studied in 10 patients, candidates for surgical treatment, prior to anaesthesia. Blood pressure was lowered to at least 50% of its initial value. In all cases, at the beginning of nitroprusside infusion, both the mean and the pulse intracranial pressures increased (mean increase: 83.2% of the initial value). At a certain moment, however, while the blood pressure continued to fall, the mean intracranial pressure did not increase any more; on the contrary, it decreased. On the other hand, in many cases, the pulse intracranial pressure continued to increase. No neurological or EEG changes were observed. The possible changes of cerebral circulation and CSF dynamics underlying the phenomena observed are discussed.
Not wonderful study shows cardene has mortality benefit over nitroprusside (NeuroCrit Care Volume 11, Number 1 2009 1556)
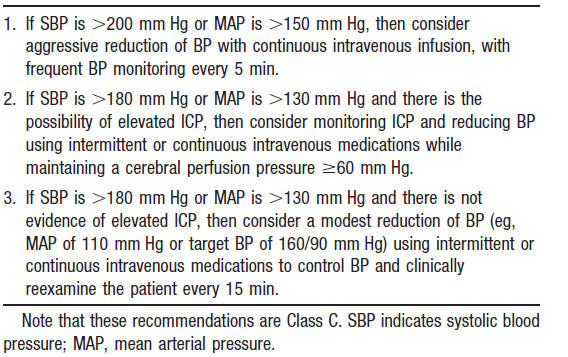
Blood Pressure Control
Interact trial You can safely lower SBP to <140, but there was not a sig. difference between this strategy and < 200 (Lancet Neurol 2008;7:391)
and in stroke
Interact2 was a negative trial for outcome or mortality (DOI: 10.1056/NEJMoa1214609)
Atach Trial (CCM Volume 38(2), February 2010, pp 637-648) states lower BPs may be safe
Better control with nicardipine vs. labetalol (neurocrit care 2013;19:41)
Newest analysis of Interact2 shows we prob. should be using 140 (Neurology February 3, 2015 vol. 84 no. 5 464-471 )
Hematoma Growth
Stroke. 1997 Jan;28(1):1-5. Links Early hemorrhage growth in patients with intracerebral hemorrhage.Brott T, Broderick J, Kothari R, Barsan W, Tomsick T, Sauerbeck L, Spilker J, Duldner J, Khoury J. University of Cincinnati Medical Center, Department of Neurology, OH 45267-0525, USA. BACKGROUND AND PURPOSE: The goal of the present study was to prospectively determine how frequently early growth of intracerebral hemorrhage occurs and whether this early growth is related to early neurological deterioration. METHODS: We performed a prospective observational study of patients with intracerebral hemorrhage within 3 hours of onset. Patients had a neurological evaluation and CT scan performed at baseline, 1 hour after baseline, and 20 hours after baseline. RESULTS: Substantial growth in the volume of parenchymal hemorrhage occurred in 26% of the 103 study patients between the baseline and 1-hour CT scans. An additional 12% of patients had substantial growth between the 1- and 20-hour CT scans. Hemorrhage growth between the baseline and 1-hour CT scans was significantly associated with clinical deterioration, as measured by the change between the baseline and 1-hour Glasgow Coma Scale and National Institutes of Health Stroke Scale scores. No baseline clinical or CT prediction of hemorrhage growth was identified. CONCLUSIONS: Substantial early hemorrhage growth in patients with intracerebral hemorrhage is common and is associated with neurological deterioration. Randomized treatment trials are needed to determine whether this early natural history of ongoing bleeding and frequent neurological deterioration can be improved.
Intraventricular Hemorrhage
Neurocritical Care © Humana Press Inc. 2008 10.1007/s12028-008-9070-2Primary Intraventricular Hemorrhage: Yield of Diagnostic Angiography and Clinical Outcome
Alexander C. Flint1 , Ashley Roebken2 and Vineeta Singh3
(1) Department of Neuroscience, Kaiser Permanente, Redwood City, 1150 Veterans Blvd, Redwood City, CA 94063, USA(2) University of California, Davis, Davis, USA(3) Department of Neurology, Neurovascular and Neurocritical Care Service, University of California, San Francisco, San Francisco, USA
Alexander C. Flint Email: alexander.c.flint@kp.org
Published online: 5 March 2008
Abstract Introduction Primary intraventricular hemorrhage (IVH), bleeding in the ventricular system without a discernable parenchymal component, is a rare neurological disorder. To better define the features of primary IVH and the yield of diagnostic angiography in this condition, we retrospectively analyzed all cases of primary IVH evaluated at a tertiary referral hospital over a 6-year period and performed a systematic review of the literature. Methods For the retrospective case series, all patients with primary IVH admitted to the neurovascular service at a single tertiary referral center over a 6-year period were identified by screening a departmental database. For the systematic review of the literature, all case series of patients with primary IVH diagnosed by computed tomography were identified in the Medline database. Results From the systematic review, the majority of patients with spontaneous primary IVH presented with headache (69%), nausea/vomiting (53%), and altered mental status (66%). Most primary IVH patients had associated hydrocephalus (62%), and about one-third required ventricular drainage (34%). Diagnostic cerebral angiography was positive for a bleeding source in 56%. The two most common causes identified by angiography were arteriovenous malformations (58% of positive angiograms) and aneurysms (36% of positive angiograms). Approximately one-third of patients with primary IVH do not survive hospital discharge (39%). Patient age and amount of IVH independently predicted in-hospital mortality. Conclusions Primary IVH is a rare form of intracerebral hemorrhage, with varying short-term outcomes that depend on patient age and the extent of intraventricular hemorrhage. The yield of diagnostic cerebral angiography in the setting of primary IVH is very high. The two most common causes of primary IVH identified on angiography are arteriovenous malformations and aneurysms. Routine catheter angiography in the setting of primary IVH is warranted. Electronic supplementary material The online version of this article (doi:10.1007/s12028-008-9070-2) contains supplementary material, which is available to authorized users.
Reversal of transtentorial herniation with hypertonic saline.
Neurology. 2008 Mar 25;70(13):1023-9. Epub 2008 Feb 13. Koenig MA, Bryan M, Lewin JL 3rd, Mirski MA, Geocadin RG, Stevens RD. Division of Neurosciences Critical Care, Johns Hopkins University School of Medicine, 600 N Wolfe St., Meyer 8-140, Baltimore, MD 21287, USA. OBJECTIVE: To evaluate the role of 23.4% saline in the management of transtentorial herniation (TTH) in patients with supratentorial lesions. METHODS: Consecutive patients with clinically defined TTH treated with 23.4% saline (30 to 60 mL) were included in a retrospective cohort. Factors associated with successful reversal of TTH were determined. RESULTS: Seventy-six TTH events occurred in 68 patients admitted with intracerebral hemorrhage (n = 29), subarachnoid hemorrhage (n = 16), stroke (n = 8), brain tumor (n = 8), subdural hematoma (n = 5), epidural hematoma (n = 1), and meningitis (n = 1). In addition to 23.4% saline, TTH management included hyperventilation (70% of events), mannitol (57%), propofol (62%), pentobarbital (15%), ventriculostomy drainage (27%), and decompressive hemicraniectomy (18%). Reversal of TTH occurred in 57/76 events (75%). Intracranial pressure decreased from 23 +/- 16 mm Hg at the time of TTH to 14 +/- 10 mm Hg at 1 hour (p = 0.002), and 11 +/- 12 mm Hg at 24 hours (p = 0.001) among 22 patients with intracranial pressure monitors. Reversal of TTH was predicted by a >/=5 mmol/L rise in serum sodium concentration (p = 0.001) or an absolute serum sodium of >/=145 mmol/L (p = 0.007) 1 hour after 23.4% saline. Adverse effects included transient hypotension in 13 events (17%); no evidence of central pontine myelinolysis was detected on post-herniation MRI (n = 18). Twenty-two patients (32%) survived to discharge, with severe disability in 17 and mild to moderate disability in 5. CONCLUSION: Treatment with 23.4% saline was associated with rapid reversal of transtentorial herniation (TTH) and reduced intracranial pressure, and had few adverse effects. Outcomes of TTH were poor, but medical reversal may extend the window for adjunctive treatments.
Surgical Intervention for ICH
STICH
Abstract Early Surgery Versus Initial Conservative Treatment in Patients With Spontaneous Supratentorial Intracerebral Haematomas in the International Surgical Trial in Intracerebral Haemorrhage (STICH): A Randomised Trial Available online 15 June 2006. Mendelow AD, for the STICH Investigators (Newcastle Gen Hosp, Newcastle upon Tyne, England; et al) Lancet. 2005;365:387-397 Background: Spontaneous supratentorial intracerebral haemorrhage accounts for 20% of all stroke-related sudden neurological deficits, has the highest morbidity and mortality of all stroke, and the role of surgery remains controversial. We undertook a prospective randomised trial to compare early surgery with initial conservative treatment for patients with intracerebral haemorrhage. Methods: A parallel-group trial design was used. Early surgery combined haematoma evacuation (within 24 h of randomisation) with medical treatment. Initial conservative treatment used medical treatment, although later evacuation was allowed if necessary. We used the eight-point Glasgow outcome scale obtained by postal questionnaires sent directly to patients at 6 months follow-up as the primary outcome measure. We divided the patients into good and poor prognosis groups on the basis of their clinical status at randomisation. For the good prognosis group, a favourable outcome was defined as good recovery or moderate disability on the Glasgow outcome scale. For the poor prognosis group, a favourable outcome also included the upper level of severe disability. Analysis was by intention to treat. Findings: 1033 patients from 83 centres in 27 countries were randomised to early surgery (503) or initial conservative treatment (530). At 6 months, 51 patients were lost to follow-up, and 17 were alive with unknown status. Of 468 patients randomised to early surgery, 122 (26%) had a favourable outcome compared with 118 (24%) of 496 randomised to initial conservative treatment (odds ratio 0.89 [95% CI 0.66-n-1.19], p=0.414); absolute benefit 2.3% (−3.2 to 7.7), relative benefit 10% (−13 to 33). Interpretation: Patients with spontaneous supratentorial intracerebral haemorrhage in neurosurgical units show no overall benefit from early surgery when compared with initial conservative treatment.
STICH II
Lancet, Volume 382, Issue 9890, Pages 397 – 408, 3 August 2013
No benefit to early surgical intervention
I believe this is Tom Bleck
Regarding treatments to stabilize the patient in order to get to the OR (or theatre for some of you, or operating department for people who object to the term room), this is one of the few circumstances in which more than modest hyperventilation is reasonable in the setting of ischemia; I might even hyperventilate more than David suggests, into the low to mid 20s for a brief period in order to get the patient to the OR. Regarding the mannitol dose, no one knows this either, but I’d probably start with 1 gm/kg on the theory that I want a high osmotic gradient and am not worried about rebound since the surgeon will make room for more swelling later. In recent years I have used a lot more hypertonic saline, but I realize that the literature is mixed in this regard; this would be a circumstance in which 30 – 60 mL of 23.4% saline (sodium quadrate in pharmacy parlance) over 10 min might be best because it seems to work most quickly. Coplin, what do you think as the holder of the IND for salt? Raise the head of the bed and give neuromuscular junction blockade so there is no coughing (boy am I old-fashioned!); there’s no point in ‘following the exam’ any longer. Turn the FiO2 up to 1.0 try to get some oxygen in without having to raise the blood pressure pharmacologically, although it is probably going up pretty high on its own (and if it isn’t, or is falling, the game is probably over already). Although there is no question that lowering core temperature lowers ICP, there isn’t time to do it here; the patient needs to be decompressed before any modality would work. I suppose I might start running in some chilled saline, which we keep around for post-cardiac arrest hypothermia, on the way to the OR, but I wouldn’t do anything that would delay transit.
I think the real question is whether to put in an external ventricular drain while the OR is being prepared. There is likely to be obstructive hydrocephalus here, and one might lower the ICP substantially by relieving it. The downside of this is the risk of upward herniation, which I have seen enough times to believe in and fear. Some folks will put one in prophylactically and clamp it to have it in place already when the patient’s exam deteriorates. If one does place an EVD, it shouldn’t be allowed to drain to atmospheric pressure; just take off a small amount of fluid. Since in the emergent situation the fluid will initially gush out, this is another argument for placing it before the patient is trying to die.
Reversal of Antiocogaulation and Antiplatelet Drugs
Lysis for Intraventricular Blood after sICH
patients did better (Stroke. 2011; 42: 2776-2781 )
Autonomic Dystability occurs if blood extends to 3rd or 4th Ventricle
(Neurocrit Care 2012;16:102)
Anticoagulation
low dose heparin can most likely be started on day 2 after ICH
Who needs an MRI
Don’t need imaging if none of the following:
- <45 y/o
- No history of HTN
- Lobar Hemorrhage
(Neurocrit Care 2013;18:59)
Interact 2 is out
Optimal achieved blood pressure in acute intracerebral hemorrhage: INTERACT2.
Abstract
OBJECTIVES:
To investigate the effects of intensive blood pressure (BP) lowering according to baseline BP levels and optimal achieved BP levels in patients with acute intracerebral hemorrhage (ICH).
METHODS:
INTERACT2 was an open, blinded endpoint, randomized controlled trial in 2,839 patients with ICH within 6 hours of onset and elevated systolic BP (SBP) (150-220 mm Hg) who were allocated to receive intensive (target SBP <140 mm Hg within 1 hour, with lower limit of 130 mm Hg for treatment cessation) or guideline-recommended (target SBP <180 mm Hg) BP-lowering treatment. Outcome was physical function across all 7 levels of the modified Rankin Scale at 90 days.
RESULTS:
Analysis of the randomized comparisons showed that intensive BP lowering produced comparable benefits on physical function at 90 days in 5 subgroups defined by baseline SBP of <160, 160-169, 170-179, 180-189, and ≥190 mm Hg (p homogeneity = 0.790). Analyses of achieved BP showed linear increases in the risk of physical dysfunction for achieved SBP above 130 mm Hg for both hyperacute (1-24 hours) and acute (2-7 days) phases while modest increases were also observed for achieved SBP below 130 mm Hg.
CONCLUSIONS:
Intensive BP lowering appears beneficial across a wide range of baseline SBP levels, and target SBP level of 130-139 mm Hg is likely to provide maximum benefit in acute ICH.
CLASSIFICATION OF EVIDENCE:
This study provides Class I evidence that the effect of intensive BP lowering on physical function is not influenced by baseline BP.
© 2014 American Academy of Neurology.
- PMID:
- 25552575
EVD Placed in the Posterior Fossa
keep no lower than 20cm to avoid upward herniation