Complete Neurologic Evaluation
Mental Status
Alert, drowsy, stuporous (pt falls asleep during exam), comatose
Lethargic-opens eyes, then falls back asleep
Obtunded-moves your hand to noxious stimuli
Stupor-general movement
Coma-nothing
GCS
Orientation
Optional: Serial 7s, Presidents, 3 objects, WORLD
Cranial Nerves
II
PERLA, Funduscopic Exam, VF (cut in half hemianopsia, homonymous or bitemporal or binasal)
1.5 mm difference in pupils is physiologic anisicoria
Papilledema-look for where vessels cross optic nerve margin, you should be able to see them sharp the whole way
III, IV, VI
EOMI, Internucleur ophthalmoplegia, abnormal adduction of ipsilateral eye from MLF lesion
III nerve palsy with preserved parasympathetics is usually from microvascular damage. If parasymp are down, think aneurysm
V
Double Stim touch on face
VII
Motor of face, can also have hyperacusis from loss of stapes dampening
Weber: place a 512 hz fork in the center of the forehead. The ear with the conduction defect will hear the sound louder
Rinne: if there is conduction defect, the sound will be louder on bone than air. Go back and forth between bone and air instead of waiting for bone to fade.
VIII
Finger rubbing
IX & X
Symmetry of palatal elevation and gag.
XI
Head turn or shoulder shrug
XII
Tongue points away from supranucleur lesion
Motor
Tone
Tremor + rigidity=cogwheeling, spasticity=velocity dependant increase in tone,
Power
0-no contraction, 1-contraction without movement, 2-partial movement c gravity eliminated, 3-movement against gravity, 4-resistance can be given, 5-normal
Pronater Drift and Gait with heels and toes and tandem
Coordination
Romberg
Intention tremor from cerebellar lesions, test c finger to nose
Dysdiadochokinesia-impairment of RAM
Abnormal Movements
Bradykinesia-decrease in normal spontaneous movements
Akinetic Mutism-extreme lack of movement or interaction
Catatonic mutism-same from schizo, may also have waxy flexibility
Dyskinesia-tardives is choreoathetoid movements of face or trunk
Choreiform-rapid movements, Athetoid-slower snake like
Akathisia-can not sit still
Most sensitive tests of corticospinal function is impairment of fine finger motions (tap forefinger and thumb) or rapid repeating hand movements
Reflexes
Frontal Release-glabellar, snout, root, grasp, palmomental reflexes indicate B frontal disease
Hoffmanns sign-clonus of upper extremity, flexion of thumb with tapping of fingers
Sensory
DSS (double simulataneous stimulation)
Exam Notation
Mental Status: Ox4, alert, appropriate affect, digits 6#«, presidents Ö, 3/3 5 min, proverbs, serial 7s
CN: II-XII intact (PERRLA, EOMI, Face/Gag/Palate symmetrical, V1-3 normal) fundi
Motor: Strengh 5/5, normal tone/bulk, no drift, F to N Ö, gait heel, toe, tandem normal, H to S normal
Sensory: vibration, pain, touch, temp, position
DTR: draw picture
NeuroOptho
monoocular diplopia or vision loss = eye or optic nerve problem
3rd nerve palsy-Eye ptosis, down & out, dilated pupil is a complete 3rd. These patients need an arterial study for aneurysm immediately
Pupil sparing=infarction, 75% diabetes 25% arthritidies. not emergent
VI is the longest course, sensitive to external compression
No such thing as a motor-sparing 3rd, must be intrinsic eye problem
The Rapid EM Neuro Exam:
Henry’s law: hear them talk, see them walk, look at their eyes.
Orientation is always lost in the same order if from organic disease:
- Time and Date
- Specific Place
Dividing line of disease
- General Place
- Name (Self)
Well cadenced, rapid speech=functioning cortex.
Ask if helicopters eat their young for hardware vs. software discrimination
Have pt close eyes and put their right thumb on their left ear and then stick out their tongue.
Facial asymmetry takes place below the nose, observe the nasolabial fold. Have patient swallow. If they are speaking to you clearly, there is no hypoglossal defect.
Pronater drift: test for 15 seconds. can not drop arm without pronation to be real weakness. Have patient close eyes, if random movements of the arms and fingers, indicates non-dominant parietal lobe dysfunction. Won’t hold arm up at all, motor impersistance=frontal lobe disease.
Reflexes:
S1S2=Ankle
L3L4=Knee
C5C6=Wrist/Hand
C7C8=elbow
note, no L5 reflex so you must have patient extend their big toe.
Rooting, snooting, grasping, sucking are frontal release signs.
Columbus award: when you don’t know where you are going, where you are, or where you have been.
Exam on Coma Patients
Dolls’ Eyes
Oculocephalic reflex or Cervico-ocular reflex
In normal, alert man, this brain-stem reflex is inhibited by gaze control mechanisms. The eyes go wherever the cortex wants them to go.
In the comatose patient, this inhibition is lost, and the oculocephalic reflex becomes disinhibited, and clinically demonstrable. Therefore, the eyes deviate in the direction opposite the head turning. This is a positive Dolls’ eyes response. Eyes stay focused on whatever they were looking at before head turning.
The brain stem has to be intact to (1) receive the afferent input of the neck stretch receptors and/or the vestibular system; (2) feed
that information to the abducens nuclei (which manage unconscious eye movements, as opposed to the pontine paramedian reticular formation, which
coordinates conscious horizontal conjugate gaze); (3) send a signal to the ipsilateral lateral rectus to abduct that eye; (4) transmit the information across the midline to the contralateral median longitudinal fasciculus, whence it goes to the horizontal component of the third nerve nucleus and
out the third nerve to adduct the contralateral eye. When you demonstrate that this reflex works in both directions, you have shown that the parts of the brainstem required to drive the cortex are intact. This means that coma is not due to a brainstem lesion but rather something higher, usually bilateral hemispheral dysfunction, rarely the diencephalon alone. QED. (cf. Parvizi J, Damasio AR. Neuroanatomical correlates of brainstem coma. Brain 2003;126:1524-1536).
Based on antique dolls that would look forward when you turn their head.
present normally, the eyes stay fixed forward c head movement, abnormal they are absent, move c head
Roberts TA, Jenkyn LR, Reeves AG. Arch Neurol 1984;41:1242-3. On the notion of doll’s eyes Buettner UW, Zee DS. Vestibular testing in comatose patients. Arch Neurol1989;46:561-3
Calorics
10 cc ice water, place head 30 degrees above supine. Slow away, then rapid back to midline. If no rapid=cerebral damage. Response named for rapid component
Glasgow Coma Scale
Points Best Eye Opening Best Verbal Response Best Motor Response6 – – Obeys 5 – Oriented Localizes pain 4 Spontaneous Confused Withdraws to pain 3 To speech Inappropriate Flexor (decorticate) 2 To pain Incomprehensible Extensor (decerebrate) 1 None None None The Glasgow Coma Scale score is determined by adding the values for eye opening, verbal response, and motor response. Possible values range from 3 to 15. Note that this scale rates the best response only. In patients who are intubated, in whom assessment of best verbal response cannot be performed, notation of this is made in the Glasgow Coma Scale score by adding a “t” to the end of the score. In patients who are intubated, the best possible score would therefore be 11t. Certain numerical values of the Glasgow Coma Scale have particular clinical significance. Patients with a Glasgow Coma Scale of 7 or less are considered to be comatose. Patients with a Glasgow Coma Scale score of 8 or less are considered to have suffered a severe head injury.

If not obeying commands- press on the supra-orbital nerve to inflict pain. If the either one hand reaches above the clavicle that scores 5 ie: localizing to pain. If the hand does not come above the clavicles but is moving towards the head, score 4 for normal flexion. If the response is a clenched fist with a flexed wrist and elbow, as in decorticate posturing, score 3. If the patient extends the elbow and flexes a clenched wrist, that is extension to pain and decerebrate posturing scoring 2. And of course no response scores 1. Pressing on nail folds is not informative as you do not know if the patient is localizing (5)or normal flexing / withdrawing (4) to pain. Besides, if that arm is paralyzed or lacks sensation secondary to a peripheral nerve injury you may misjudge the GCS. (Narani)
A topic close to my heart. GCS is often very poorly assessed, and interindividual difference can be spectacular. It fascinates me to see a previously stable GCS suddenly change by a number of units at the time of a nursing shift handover! A. Central pain needs to be central and specific. By far the best is the supraorbital nerve. Another reasonable site is a trapezius squeeze. The ‘sternal rub’ is useless, non specific and also disfiguring (how many times have you seen bruising after too many people have done misguided, violent sternal rubs). I threaten to break the arms of any of my own staff I see doing it. Attached find a picture of a patient who had one too many vigorous sternal rubs. The supraorbital nerve is also the only specific way to distinguish between appropriate (M4) and inappropriate flexion (M3) and localisation (M5), depending on whether the hand comes ABOVE the clavicle [need to come above the clavicle to score a 5] B. It is part of your overall neurological assessment of a patient, which includes an examination to rule out spinal cord injury. I have attached the original description of the motor response from Teasdale and Jennett. C. Hourly / 4th hourly GCS is of much less value in a sedated patient. One of the standard ‘errors’ in APACHE II scoring is to assign a GCS3 to someone deeply sedated and unresponsive (=12 points instantly!). A great way to dishonestly bring down your SMR and one thing I specifically look at when assessing a unit’s data during training accreditation inspections. I note your question refers to ongoing GCS assessments in ICU – that is a different animal to a one off assessment in the emergency department, and the reproducibility of ICU observations is paramount (rather than the ‘best’ response per se) Cheers, Ian Ian Seppelt FANZCA FJFICM
Thomas Bleck <tbleck@gmail.com> Posturing or localization in response to any noxious stimulus, face or trunk or extremities, provides important information on what parts of the brainstem are working (flexion = rubrospinal system in control of the spinal cord, extension = vestibulospinal system in control, no arm movement but knee flexion, medullary centers still working after vestibular efferents lost). As I mentioned before, there are occasional patients who do nothing in response to nailbed pressure but who extend, flex, or even localize with a sternal rub. So while I don’t do a sternal rub if I get a reproducible response to nailbed pressure in a comatose patient, I do perform the sternal rub if other stimuli below the neck have not elicited anything.
Adie’s Pupil
Classically, the affected pupil will be larger than the fellow eye, and exhibit a sluggish reaction to light. The pupil will react vigorously to near stimuli but the near response is tonic, meaning the miosis persists longer in the affected eye with slow redilation after removal of the near stimulus. Adie’s pupil is most often found in young women and is associated with a generalized loss of deep tendon reflexes. Frequently, patellar and Achilles reflexes are absent. There is a feeling that light is too bright in the affected eye (because the pupil helps to reduce light intensity by constricting in bright light). The condition is believed to result from damage to the cilliary ganglion caused by infectious (viral) or vascular disease. Adie’s pupil is supersensitive to dilute solutions of pilocarpine and can be positively identified if 1/8% pilocarpine constricts the pupil (this will not constrict a normal pupil, such as in the patient with a third cranial nerve palsy as the etiology of anisocoria). (Emedhome.com)
Quick Motor Exam
Tone
Pronator Drift
F to N
Fine Finger Motion
Hand Bulk
Finger Extensor strength and intrinsic muscle strength of finger spread
Babinski
not sensitive and its LRs make it fairly useless. Speed of foot tapping is more demonstrative of UMN lesion. Slowed foot is sign of the lesion. (Neurology Volume 65(8), 25 October 2005, pp 1165-1168)
Ptosis
To examine the levator palpebrae muscle, note is made of the portion of the iris that is covered by the upper lid, and compared with the opposite side. Ptosis can be exaggerated by having the patient look up. If ptosis is present, the patient should be tested for lid fatigue: the ptosis may worsen when the patient refrains from blinking for a time or attempts to maintain upgaze. Ptosis from myasthenia gravis is often asymmetric, fatigable, and improves with short periods of rest (4). Other conditions causing ptosis include Horner’s syndrome, botulism (or injection of botulinum toxin), palpebral trauma, and cluster headache; ptosis also may be congenital (5). Pseudoptosis is caused by enopthalmos (e.g., from an orbital blowout fracture), which makes the lid seem to be relatively lower on the side with the sunken globe. (JEM 2008)
The Brainstem from Life in the Fast Lane & Chris Nickson
Brainstem Rules of 4
Hands up who enjoyed learning the anatomy of the brainstem in medical school?
Hmm, thought so.

In 2005, Peter Gates published a superb paper titled:
The rule of 4 of the brainstem: a simplified method for understanding brainstem anatomy and brainstem vascular syndromes for the non-neurologist.
Gates described a simplified method for answering the question Where is the lesion? using only the parts of the brainstem that we actually examine during a clinical examination to understand brainstem vascular syndromes.
Firstly, a quick review of the blood supply of the brainstem. Simply put the blood supply comes from:
- paramedian branches
- long circumferential branches (SAP)
- superior cerebellar artery (SCA)
- anterior inferior cerebellar artery (AICA)
- posterior inferior cerebellar artery (PICA)
And occlusion of these two groups of vessels results in two distinct types of brainstem syndrome:
- medial (or paramedian) brainstem syndromes( due to para-median branch occlusion)
- lateral brainstem syndromes( due to occlusion of the circumferential branches, also occasionally seen in unilateral vertebral occlusion)
And now the rules. If you can remember these rules the diagnosis of brainstem vascular syndromes becomes a pitifully simple exercise (?!) heres how it works:
In the rule of 4 there are 4 rules
- There are 4 structures in the midline beginning with M
- There are 4 structures to the side (lateral) beginning with S
- There are 4 cranial nerves in the medulla, 4 in the pons and 4 above the pons (2 in the midbrain)
- The 4 motor nuclei that are in the midline are those that divide equally into 12 except for 1 and 2, that is 3, 4, 6 and 12(5, 7, 9 and 11 are in the lateral brainstem)
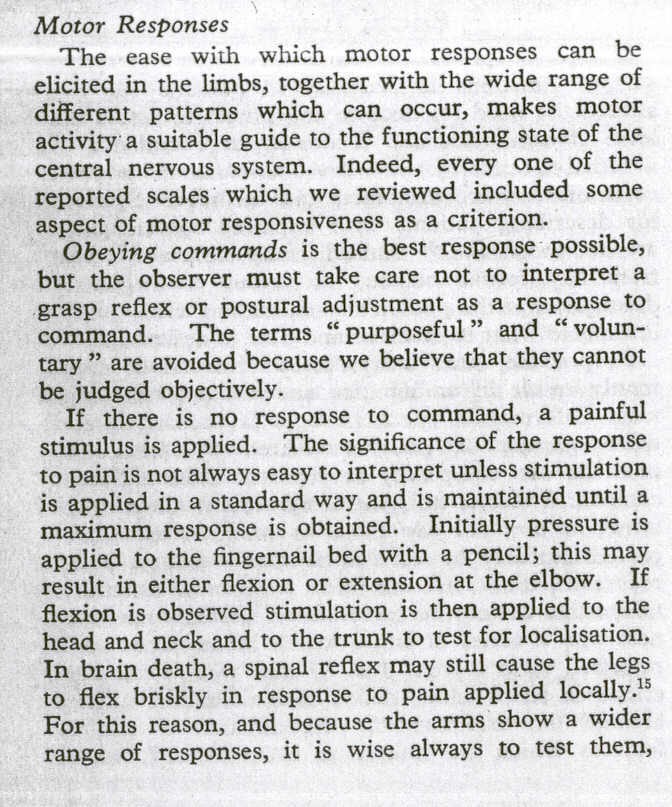
The 4 medial structures and the associated deficits are:
- Motor pathway (or corticospinal tract): contralateral weakness of the arm and leg
- Medial Lemniscus:contralateral loss of vibration and proprioception in the arm and leg
- Medial longitudinal fasciculus:ipsilateral inter-nuclear ophthalmoplegia(failure of adduction of the ipsilateral eye towards the nose and nystagmus in the opposite eye as it looks laterally)
- Motor nucleus and nerve:ipsilateral loss of the cranial nerve that is affected (3, 4, 6 or 12)
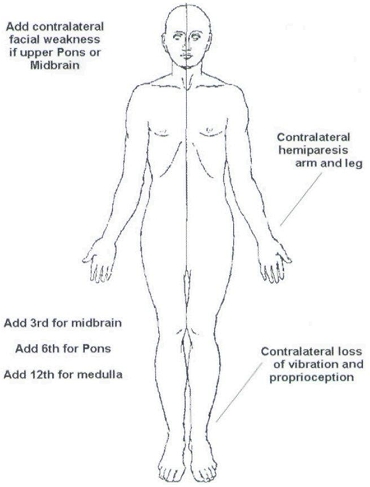
The 4 side (lateral) structures and the associated deficits are:
- Spinocerebellar pathway:ipsilateral ataxia of the arm and leg
- Spinothalamic pathway:contralateral alteration of pain and temperature affecting the arm, leg and rarely the trunk
- Sensory nucleus of the 5th cranial nerve: ipsilateral alteration of pain and temperature on the face in the distributionof the 5th cranial nerve(this nucleus is a long vertical structure that extends in the lateral aspect of the pons down into the medulla)
- Sympathetic pathway:ipsilateral Homers syndrome, that is partial ptosis and a small pupil (miosis)
According to Gates:
These pathways pass through the entire length of the brainstem and can be likened to meridians of longitude whereas the various cranial nerves can be regarded as parallels of latitude. If you establish where the meridians of longitude and parallels of latitude intersect then you have established the site of the lesion.
The 4 cranial nerves in the medulla are CN9-12:
- Glossopharyngeal (CN9):ipsilateral loss of pharyngeal sensation
- Vagus (CN10):ipsilateral palatal weakness
- Spinal accessory (CN11):ipsilateral weakness of the trapezius and stemocleidomastoid muscles
- Hypoglossal (CN12):ipsilateral weakness of the tongueThe 12th cranial nerve is the motor nerve in the midline of the medulla. Although the 9th, 10th and 11th cranial nerves have motor components, they do not divide evenly into 12 (using our rule) and are thus not the medial motor nerves.
The 4 cranial nerves in the pons are CN5-8:
- Trigeminal (CN5):ipsilateral alteration of pain, temperature and light touch on the face back as far as the anterior two-thirds of the scalp and sparing the angle of the jaw.
- Abducent (CN6):ipsilateral weakness of abduction (lateral movement) of the eye (lateral rectus).
- Facial (CN7):ipsilateral facial weakness.
- Auditory (CN8):ipsilateral deafness.The 6th cranial nerve is the motor nerve in the medial pons.The 7th is a motor nerve but it also carries pathways of taste, and using the rule of 4 it does not divide equally in to 12 and thus it is not a motor nerve that is in the midline.The vestibular portion of the 8th nerve is not included in order to keep the concept simple and to avoid confusion. Nausea and vomiting and vertigo are often more common with involvement of the vestibular connections in the lateral medulla.
The 4 cranial nerves above the pons are CN1-4:
- Olfactory (CN1):not in midbrain.
- Optic (CN2):not in midbrain.
- Oculomotor (CN3):impaired adduction, supradduction and infradduction of the ipsilateral eye with or without a dilated pupil. The eye is turned out and slightly down.
- Trochlear (CN4):eye unable to look down when the eye is looking in towards the nose (superior oblique).The 3rd and 4th cranial nerves are the motor nerves in the midbrain.
Thus a medial brainstem syndrome will consist of the 4 Ms and the relevant motor cranial nerves, and a lateral brainstem syndrome will consist of the 4 Ss and eitherthe 9-11th cranial nerve if the lesion is in the medulla, or the 5th, 7th and 8th cranial nerve if the lesion is in the pons.
Handy tip:If there are signs of both a lateral and a medial (paramedian) brainstem syndrome, then one needs to consider a basilar artery problem, possibly an occlusion.
Ill let you mull over these rules until the next brainstem post, where youll be able to test drive Gates Brainstem Rules of 4′ on some clinical scenarios.
References
- Gates, P. The rule of 4 of the brainstem: a simplified method for understanding brainstem anatomy and brainstem vascular syndromes for the non-neurologist. Internal Medicine Journal 2005; 35: 263-266 [pubmed]
- Goldberg, S. Clinical Neuroanatomy Made Ridiculously Simple. MedMaster Series, 2000 Edition. [betterworldbooks]
Circle of Willis Mnemonic
from lifeinthefastlane.com
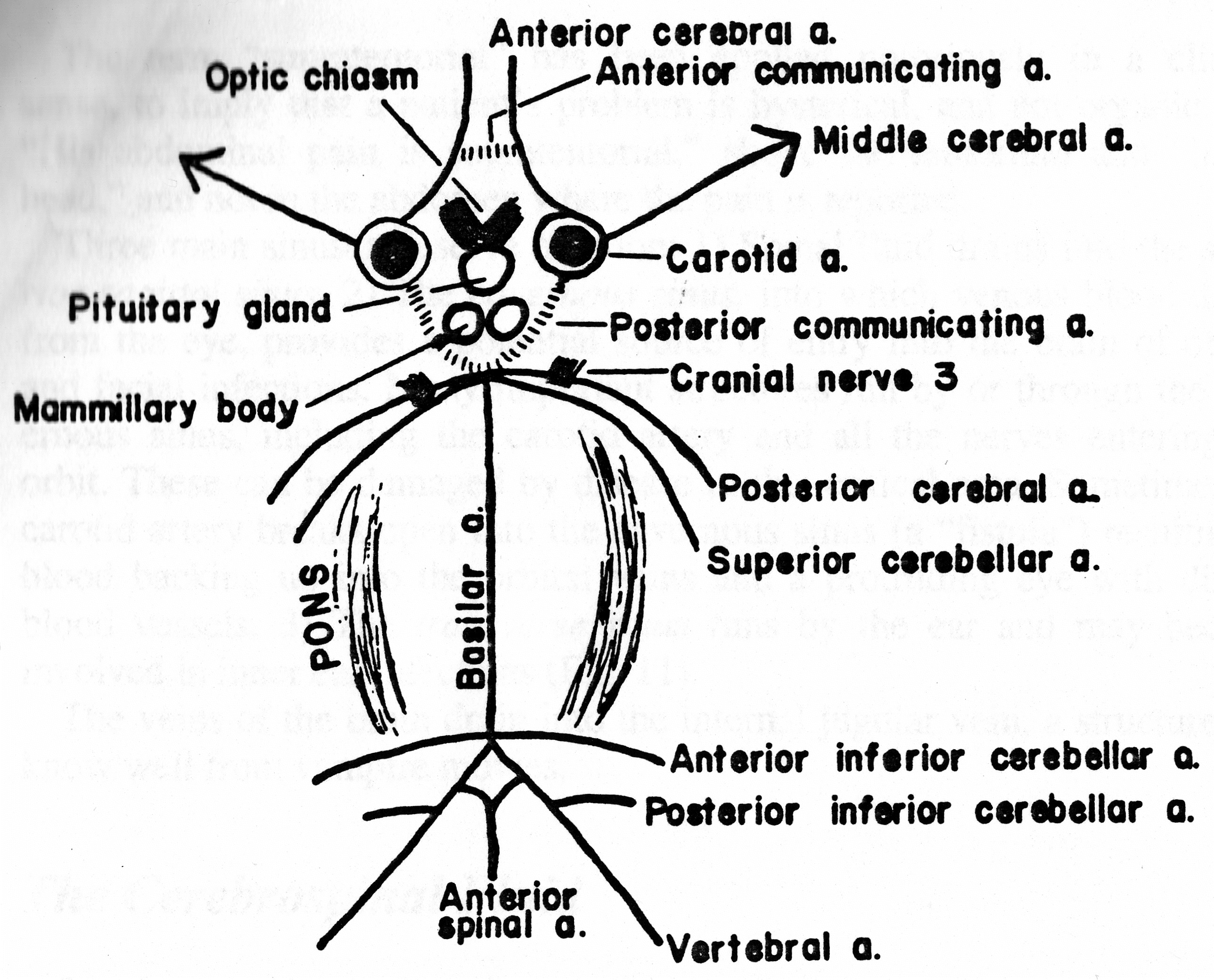
A ferocious spider lives in the brain. His name is Willis!
Note that he has a nose [pituitary gland], two suckers [mamillary bodies], eyes that look outward [internal carotid arteries], a crew cut [anterior communicating artery – blood flows in either direction], antennae [anterior cerebral arteries], a fuzzy beard [posterior communicating arteries – again, blood flows in either direction], 8 legs, a belly that, according to your point of view, is either thin (basilar artery) or fat (the pons, which lies from one end of the basilar artery to the other), two feelers on his rear legs [posterior inferior cerebellar arteries], and male genitalia [anterior spinal artery].
Willis has hairy armpits the third cranial nerve exists between the posterior cerebral artery and the superior cerebellar artery [the first two sets of legs].
The cerebellar arteries were named by a real SAP (S superior, A anterior inferior, and P posterior inferior) [SA – the last two sets of legs] and supply the cerebellum and brainstem.
References
- Goldberg, S. Clinical Neuroanatomy Made Ridiculously Simple. MedMaster Series, 2000 Edition.
From Chris Nickson and LitFL Blog
aka Neurological Mind-boggler 007
You are reviewing an unconscious patient in the emergency department. Meanwhile, the resus team is preparing to intubate the patient for airway protection prior to facilitate transfer to CT.
See Neurological Mind-boggler 005 for an approach to the differential diagnosis of coma (Q1) and abnormally sized pupils (Q2)
Questions
Q1. What are the 5 key components of the neurological examination of the comatose patient?
According to Posner et al (2008), the key components of the neurological examination of the comatose patient are:
- level of consciousness (Glasgow Coma Score list the components; e.g. E4V5M6 = GCS 15)
- the pattern of breathing
- size and reactivity of the pupils
- eye movements and oculovestibular responses
- motor responses (tone, reflexes and posturing)
These can be rapidly assessed in a few minutes. I would also add to check for evidence of meningism, and emphasize the search for focal neurological deficits.
General examination is also important consider the neurological findings in light of the vital signs, evidence of trauma, acute or chronic illness, and/or drug ingestion.
The patient is GCS3, has a slow but otherwise unremarkable pattern of breathing and the pupils are midsized, equal and reactive. Tone and reflexes are normal and there is no abnormal posturing.
Next you assess the patients corneal reflexes and spontaneous eye movements.
Q2. What is the significance of the eyes rolling up on corneal stimulation?
Upward rolling of the eyes (with reflexive eyelid closure) on corneal stimulation implies that the pons and midbrain are intact (the reflex pathway involves the trigeminal nerve, the spinal CN5 nucleus, the lateral brainstem tegmentum, and the CN3 and CN7 nuclei if necessary revise the Brainstem Rules of 4).
If the eye turns upwards but the eyelid does not close there is a CN7 lesion (Bells phenomenon).
If the eye does not turn upwards and the eyelid does not close there is a CN5 lesion.
Loss of the corneal reflex is usually a late sign in coma.
To avoid corneal trauma in the unconscious patient, corneal stimulation can be performed by dropping a few drops of sterile saline onto the cornea from a height of 10 cm.
Patients that chronically wear contact lenses may have diminished corneal reflexes.
Q3. What lesion should be suspected if the eyes are tonically deviated to the left?
This is suggestive of either:
- A frontal lobe lesion on the same side as the eye deviation, commonly a stroke.This can also be a result of a Todds paralysis following a seizure (whereas during the seizure the eyes deviate in the opposite direction away from the origin of the irritative focus).
or
- A pontine lesion on the opposite side to the eye deviation.Wrong way eyes may also be seen in thalamic hemorrhage.
Lateral gaze deviation from a pontine lesion cannot be overcome by stimulating oculocephalic or ocularvestibular reflexes (see below), whereas supranuclear (e.g. frontal lesions) can. Hence they can be distinguished clinically.
Q4. What lesion should be suspected if there is vertical separation of the ocular axes?
Vertical separation of the ocular axes is called skew deviation. This is suggestive of a pontine or vestibulo-cerebellar lesion on the side of the inferior eye, or a medial longitudinal fasciculus lesion on the side of the superior eye.
On examining the patients eyes, he appears to resist eye opening. When opened he has saccadic eye movements. The eyelids once opened stayed open, they did not close smoothly and gradually.
Q5. What are the different types of spontaneous eye movement seen in comatose patients and what do they indicate?
Eye movements seen in the comatose patient include:
- roving eye movements Description: slow random predominantly horizontal conjugate eye movements (though there may be a degree of exophoria) similar to those seen in deep sleep.Likely cause: metabolic encephalopathy (may be absent in deep coma), bilateral supranuclear lesions
- ocular bobbing Description: Rapid, conjugate, downward movement; slow return to primary position Likely cause: Pontine strokes; other structural, metabolic, or toxic disorders
- ocular dipping Description: Slow downward movement; rapid return to primary positionLikely cause: Unreliable for localization; follows hypoxic-ischemic insult or metabolic disorder
- reverse ocular bobbing Description: Rapid upward movement; slow return to primary positionLikely cause: Unreliable for localization; may occur with metabolic disorders
- reverse ocular dipping Description: Slow upward movement; rapid return to primary positionLikely cause: Unreliable for localization; pontine infarction and with AIDS
- ping-pong gaze Description: Horizontal conjugate deviation of the eyes, alternating every few seconds Likely cause: metabolic encephalopathy, bilateral cerebral hemispheric dysfunction; toxic ingestion
- periodic alternating gaze deviation Description: Horizontal conjugate deviation of the eyes, alternating every 2 minutesLikely cause: Hepatic encephalopathy; disorders causing periodic alternating nystagmus and unconsciousness or vegetative state
- vertical myoclonus Description: vertical pendular oscillations (23 Hz)Likely cause: Pontine strokes
- horizontal myoclonus Description: rapid horizontal pendular oscillations; the eyes appear to be shaking. Likely cause: Serotonin toxicity
- monocular eye movements Description: Small, intermittent, rapid monocular horizontal, vertical, or torsional movementsLikely cause: Pontine or midbrain destructive lesions, perhaps with coexistent seizures
Most individuals have a degree of exophoria when drowsy for any reason and any underlying strabismus tends to worsen thus dysconjugate gaze is difficult to interpret in the stuporose or comatose patient.
A simplified approach to spontaneous eye movements in coma is:
- roving eye movements metabolic/ toxic encephalopathy most likely, or although they can also occur with bilateral lesions above the brainstem.
- other weird and wonderful eye movements structural, metabolic or toxicological cause of comas.
- saccadic eye movements or fixing and following pseudocoma (feigned coma).
Q6. How can pseudocoma (a patient feigning coma) be differentiated from true coma?
Pseudocoma is a diagnosis of exclusion. The following features are consistent with pseudocoma:
- The pattern of clinical findings are not consistent with a specific neurological syndrome or anatomical lesion.
- Pupils:
- pupils are equal and reactive to light.
- passive eyelid opening results in pupillary constriction, whereas if the patient is sleeping or comatose (with intact pupillary reflexes) the pupils dilate on passive eyelid opening.
- Eye movements and oculovestibular reflexes:
- fluttering of the eyelids when the eyelashes are gently stroked
- the patient may resist passive eye opening. Occasionally patients with metabolic or structural lesions may resist eye opening.
- any spontaneous eye movements are saccadic (rapid and jerking) rather than slowly roving
- the patient actually makes eye contact with the examiner when the eyelids are opened; or the eyes always look to the side away from the examiner, or the eyes always look towards the ground
- the awake patients eyes move concomitantly with head rotation when assessing the oculocephalic reflex. It is nearly impossible for an awake patient to mimic the brainstem oculocephalic responses of a truly comatose patient.
- on cold caloric testing the patient may wake up or exhibit preservation of the fast component of nystagmus.
- Motor
- active resistance or varying resistance to passive motor tone testing, or cog-wheeling resistance with sudden giving-away phenomena
- no abnormal reflex posturing in response to painful stimuli
- the patient may occasionally make voluntary movements or change body position in bed
- the patient will show avoidance of self injury do not allow the patient to be injured!
Q7. How are oculcephalic and oculovestibular reflexes tested?
Oculocephalic reflex:
- ensure the C-spine is cleared.
- the patients eyes are held open.
- the head is briskly turned from side to side with the head held briefly at the end of each turn.
- a positive response occurs when the eyes rotate to the opposite side to the direction of head rotation, thus indicating that the brainstem (CN3,6,8) is intact.
- a similar result is seen when the head is flexed and extended a positive result is downward deviation of the eyes during extension, and upward deviation during flexion (the eyelids, if closed, may also open as part of the dolls head phenomenon). These vertical responses indicates that the brainstem (CN3,4,8) is intact.
- The eyes should gradually return to the mid-position in a smooth, conjugate movement if the brainstem is intact.
Patients with metabolic coma (e.g. hepatic failure) may have exaggerated, brisk oculocephalic reflexes.
Oculovestibular reflex (caloric stimulation):
- the head is elevated to 30 degrees above horizontal so that the lateral semicircular canal is vertical, and so that stimulation with generate a maximal response.
- check that the tympanum is intact and that the external ear canal is clear C-spine clearance is not necessary.
- introduce iced water into the external ear canal through a small cather until one of the following occurs:
- nystagmus (in the intact brainstem the slow phase is towards the irrigated ear)
- ocular deviation
- 200mL of iced water has been instilled.
- allow 5 minutes between testing ears to allow re-equilibration of the oculovestibular system.
- as consciousness is lost, the fast component (towards the non-irrigated ear) is lost and the slow component tonically deviates the eye in the direction of the irrigated ear.
Vertical oculo-vestibular eye responses can be assessed by irrigated both ears simultaneously. If the brainstem is intact, cold water causes the eyes to deviate downwards and warm water causes the eyes to deviate upwards.
The positive brainstem responses described above are those seen in a comatose patient with an intact brainstem. As described in Q4, results in an awake patient with an intact brainstem may differ
Brainstem encephalitis, deep metabolic coma and certain drugs may mimic brainstem death. such drugs include recently administered antiepileptics such as phenytoin and barbiturates. Like phenytoin, tricyclic overdose may cause bilateral vestibular failure, as might aminoglycoside vestibulotoxicity. Baclofen overdose can also mimic brain death.
Another caveat pertains to the trauma patient ocular movements may be impaired if a blowout fracture has trapped the extraocular muscles.
Typical findings for various lesions are shown in this graphic from Posner et al (2008):

Click to enlarge
Q8. What is Colliers sign?
Tonically retracted eyelids occasionally seen in patients with dorsal midbrain or pontine lesions.
Now that you know, you can forget about it
Q9. What are the two most important findings to look for on fundoscopy of the undifferentiated coma patient?
Id put these two at the top of the list:
- papilloedema optic disc swelling due to raised intracranial pressure. However, the absence of papilloedema does not rule out intracranial hypertension
- evidence of Terson syndrome vitreous, subhyaloid, or retinal bleeding in association with subarachnoid hemorrhage.
References
- Bersten AD, Soni N. Ohs Intensive Care Manual (6th edition). Butterworth-Heinemann, 2008.
- Jeff Manns EM Guidemaps. Coma.
- Poser JB, et al. Plum and Posners Diagnosis of Stupor and Coma (4th edition), Oxford university Press, 2007.
From LitFL Blog and Chris Nickson
Look left, look right
from Life in the Fast Lane by Chris Nickson
aka Neurological Mind-boggler 008
An elderly Scottish lady presented to the emergency department following a fall. Apart from a few minor scrapes she came through the ordeal relatively unscathed. However, examination of her ocular movements demonstrated an abnormal finding.
She was asked to look to her right:

Click to enlarge
And to her left:

Click to enlarge
Q1. Describe the clinical finding.
When the patient was asked to look right, there was voluntary conjugate deviation of the eyes to the right. However, when she was asked to look to the left, the left eye abducted but the right eye failed to adduct it did not move past the midline.
In addition, although not shown in these images, horizontal nystagmus was noted in the left eye when the the patient was asked to look to her left.
Q2. What is the name of the this clinical finding?
Unilateral internuclear ophthalmoplegia (INO) affecting the right eye.
In INO, when the patients gaze is directed away from the side of the lesion, the ipsilateral (adducting) eye will not adduct and the contralateral (abducting) eye demonstrates horizontal nystagmus.
Surprisingly, pateints with INO do not usually complain of diplopia!
Q3. Where is the anatomical lesion?
Internuclear ophthalmoplegia (INO) is caused by a lesion in the medial longitudinal fasciculus (MLF).
The MLF provides a connection between CN3 nucleus in the midbrain (and, therefore, the medial rectus) and the CN6 nucleus in the pons (abducens) on the opposite side and facilitates conjugate eye movements on lateral gaze.
Abduction in either eye is normal, whereas adduction is impaired, resulting in dissociation of eye movements in other words the eyes move independently on lateral gaze. When each eye is tested independently by covering the other eye, medial rectus function is shown to still be present. Saccades may be slow before adduction is impaired.
In this case, the lesion is affecting the MLF between the left CN6 nucleus and the right CN3 nucleus.
Q4. What are the possible causes of this clinical finding?
Causes of internuclear ophthalmoplegia (INO) include:
- Multiple sclerosis
likely cause in adulthood/middle age; often bilateral.- Vascular brainstem lesion
likely cause in the elderly or people with vascular risk factors; often unilateral.- Pontine glioma
more likely cause in children.- Inflammatory encephalitis affecting the brainstem (e.g. autoimmune, infective)
- Myasthenia gravis (unusual)
Bilateral INO is nearly pathognomonic for multiple sclerosis.
Q5. What is a one-and-a-half syndrome?
The one-and-a-half syndrome is an internuclear ophthalmoplegia combined with a conjugate gaze paralysis in the other direction. One eye fails to adduct on attempted lateral gaze (the half) and the other eye neither adducts nor abducts (the one). The eye that can abduct may exhibit horizontal nystagmus when it does so.
The responsible lesion is an extensive paramedian pontine lesion that involves the MLF and either the CN6 nucleus or the PPRF (parapontine reticular formation). If the INO affects the left eye, the lesion is on the right (same side as the eye with the complete conjugate gaze palsy).
The PPRF is the brainstem gaze center that controls horizontal gaze. It innerves the CN6 nucleus and receives projections from higher centers including the contralateral frontal eye fields. An ipsilateral gaze palsy results from a lesion in either the PPRF or the CN6 nucleus.
One-and-a-half syndrome usually occurs in conjunction with other brainstem symptoms and signs.
The causes of one-and-a-half syndrome include:
- Brainstem infarction
most common cause in the elderly.- Multiple sclerosis
most common cause in young adults.- Trauma
- Postoperatively after posterior fossa procedure
- Basilar artery aneurysm or brainstem arteriovenous malformations
- Myasthenia gravis
pseudo one-and-a-half syndrome
References
- Bhidayasiri R, Waters MF, Giza CC. Neurological differential diagnosis: a prioritized approach, Blackwell Publishing 2005.
- Duong DK, Leo MM, Mitchell EL. Neuro-ophthalmology. Emerg Med Clin North Am. 2008 Feb;26(1):137-80, vii. PMID: 18249261.
- Patten J. Neurological differential diagnosis (2nd edition), Springer-Verlag 1996.
To test for true (ankle) clonus:
Elicit such in the usual fashion (forcibly dorsiflex the foot). If clonus begins, then, keeping the foot dorsiflexed, plantar flex the great toe. If the clonus is true, this will stop it.
Frontera Additions
people like to track faces and money, but not fingers
have patient count backwards from 20 to 1, trend this
| | |