

From Anaestricks
Unless you do a lot of paediatrics, you often don’t think about the dose of blood products by body weight, and they can sometimes be difficult to find.
- Red Cells: 4ml X kg X Hb g/dL rise required. (1 unit/bag ~ 300mL)
- Fresh frozen plasma: 10 – 20 ml/kg (1 bag ~ 230mL)
- Cryoprecipitate: 5-10 ml/kg (1 bag ~ 20mL)
- Platelets: 10ml/kg (1 unit ~ 60mL. 1 pooled bag = 5 units)
- Tranexamic acid: 100mg/kg then 10mg/kg/hr
- Factor 7: 90mcg/kg
- Prothrombin (factor 9) complex: 1mL/kg (25units/kg)
PS – To make it easier to remember: FFP, cryo and platelets are all about 10ml/kg.
Risks of Transfusion
from emedhome
Current Estimated Risks of Blood Transfusion
Emergency Physicians often order blood transfusions in the ED and face questions from patients, family members, and staff regarding the risks. This clinical pearl is meant as a reference to outline the current estimated risks. The main reason today for transfusion-transmitted infection is the window period when a donor may be infectious, but the particular agent is not yet present at a detectable level. For example, even the most sensitive screening technologies currently available cannot identify the presence of HIV infection during the first few days after infection, when neither HIV RNA nor HIV-specific antibodies have reached detectable levels (1).
- HIV – The estimated risk for acquiring HIV infection today is 1 in 1,467,000 transfused blood components (2,3).
- HCV – The estimated risk is 1 in 1,149,000 transfused blood components (2,3).
- HBV – The estimated risk for HBV is 1 in 282,000 to 1 in 357,000 transfused blood components (3,4). As recently as 1999, the risk was approximately 1 in 86,000.
- Transfusion-Related Acute Lung Injury – Although the literature offers a wide range of TRALI risk estimates, in a recently-published, large, prospective study, the rate of TRALI occurrence was 8.1 per 100 000 transfused blood components (5).
- Fatal Hemolysis – Transfusion-related fatalities due to hemolysis reported to the FDA averaged 12.5 deaths/yr from 2005- 2010 (3). With 15 million RBC units transfused per year, the estimated risk for death due to hemolysis is 1:1,250,000.
References:
(1) MMWR Weekly October 22, 2010 / 59(41);1335-1339.
(2) Zou S, et al. Transfusion 2010; 50:1495-504.
(3) Carson JL, et al. Ann Int Med 2012;157(1):49-58.
(4) Zou S, et al. Â Transfusion 2009;49(8):1609-20.
(5) Toy P, et al. Blood 2012; 119:1757-1767.
Whole Blood
used in Iraq conflict with great success
Packed Red Blood Cells (PRBC)
1 unit is ~250-300 cc including citrate preservative; it has a crit of ~70%
Storage life is ~30 days
can add saline to speed infusion
HCT of 70%
Each unit may have 2-4 grams of particulate matter which may overwhelm the filters.
When you ask for large numbers of units, the blood bank will dump all of its old blood. Old blood has citrate and ammonia in it. Low 2-3 BPG levels prevent unloading of peripheral oxygen.
If you give more than 4 units of untyped, can run into problems due to Anti-A or B antibodies in the blood itself.
Massive transfusions (10 units in 6-12 hours) cause hyperkalemia, hypocalcemia, hypothermia, coagulopathy, and immunosuppresion.
Do not autotransfuse more than 6 units.
Do not give FFP or Plt unless massive bleeding or coagulopathy
leukocyte filtered blood can reduce fever from transfusion
washed blood removes the plasma/preservative solution
Storage time does not effect the tissue oxygenation of red blood cells from 5 day old vs. 20 day old (Crit Care Med 2004 32:2. p.364)
transfusion of non-filtered packed red cells may cause leukocytosis, this effect is eliminated if blood is filtered prior to storage. (Crit Care Med 2004 32:2)
One unit of red blood cells (RBC) contains approximately 200mL red blood cells, 100 mL Optisol AS-5® (a solution added to extend storage life) and ~30mL plasma
Should raise crit ~3%
Scalea studied safety of uncrossmatched O blood transfusions; it appears to be safe with low risk of Rh- patient reactions to positive blood (J Trauma 2005;59:1445)
Blood Transfusion
Infusing LR with blood did not cause clots (Am J Surg 1998;175:308)
NO deficiency probably causes the poor O2 carrying capacity of banked blood; putting NO in before transfusion may ameloriate this response (PNAS 2007;104(43):17058)
you can use type O + without a second thought (Surg Gynecol Obstet 167(3):229 1988)
Incredible review of transfusions for SAH which also touches on many of the issues of old blood
Fresh Frozen Plasma (FFP)
ffp has an inr of 1.6; All the FFP in the world will not reduce the INR below this point (Am J Clin Path 2006;126(1):133)
$1 per ml when you factor in extra costs
1 unit per ml of each factor
The usual volume of 1 unit is 220-250 cc
Vitamin K dependent factors in concentration of 1 Unit/cc
approx $1 per ml when you factor in extra costs
FFP has an INR of 1.5
FFP must be ABO compatible
Give 2-4 units
10-20 cc/kg (4-6 units in adults) will increase factros by ~20%
- Toward rational fresh frozen plasma transfusion: the effect
of plasma transfusion on coagulation test results. Am J Clin Pathol
126(1):133-139, 2006. - Effect of fresh frozen plasma transfusion on prothrombin time
and bleeding in patients with mild coagulation abnormalities.
Transfusion 46(8):1279-1285, 2006.
Fresh Frozen Plasma (FFP) Description One unit of FFP or thawed plasma is the plasma taken from a unit of whole blood. It is frozen within eight hours of collection. FFP contains all coagulation factors in normal concentrations. Thawed plasma may be transfused up to 5 days after thawing and contains slightly decreased levels of Factor V (66+-9%) and decreased Factor VIII levels (41+-8%). Plasma is free of red blood cells, leukocytes and platelets. One unit is approximately 250mL and must be ABO compatible. Rh factor need not be considered. Since there are no viable leukocytes, plasma does not carry a risk of CMV transmission or Graft Vs. Host Disease (GVHD). Indications Plasma transfusion is indicated in patients with documented coagulation factor deficiencies and active bleeding, or who are about to undergo an invasive procedure. Deficiencies may be congenital or acquired secondary to liver disease, warfarin anticoagulation, disseminated intravascular coagulation, or massive replacement with red blood cells and crystalloid/colloid solutions. FFP should not be used for Hemophilia B (Factor IX) deficiency unless Factor IX concentrate is not available. FFP, but not thawed plasma, can be used for Factor V deficiency. Recombinant or Factor VIII concentrates should be used to replace Factor VIII. Usually, there is an increase of at least 1.5 times the normal PT or PTT or an INR ≥ 1.6 before clinically important factor deficiency exists. This corresponds to factor levels <30% of normal. Reversal of warfarin anticoagulation with plasma is indicated only if significant bleeding or risk is present. Often it will require recurrent transfusion to maintain normal factor levels. Otherwise, reversal can be achieved by giving Vitamin K two to three days prior to a planned procedure. Rapid reversal for life threatening bleeding may be achieved with recombinant Factor VIIa (Novo7®) or PCC Plasma is indicated in the treatment of thrombotic thrombocytopenic purpura (TTP), usually in conjunction with plasma exchange. Plasma should not be used for volume expansion unless the patient also has a significant coagulopathy and is bleeding. Plasma – Dosage Volume of 1 Unit Plasma: 200-250 mL 1 mL plasma contains 1 u coagulation factors 1 Unit contains 220 u coagulation factors Factor recovery with transfusion = 40% 1 Unit provides ~80 u coagulation factors 70 kg X .05 = plasma volume of 35 dL (3.5 L) 80 u = 2.3 u/dL = 2.3% (of normal 100 u/dL) 35 dL each unit contains 13 mg/dl of fibrinogen
In a 70 kg Patient: 1 Unit Plasma increases most factors ~2.5% 4 Units Plasma increase most factors ~10% Therapeutic Effect Usually an increase in factor levels of at least 10% will be needed for any significant change in coagulation status, so the usual dose is four units, but the amount will vary depending on the patient’s size and clotting factor levels. Hematology consultation is advised concerning the dose of plasma. Recommended Coagulation Parameters for Common Procedures Platelet Count* INR Lumbar Puncture ≥50,000 ≤1.5 Paracentesis ≥30,000 ≤2.0 Thoracentesis ≥50,000 ≤1.5 Transbronchial Lung Biopsy ≥50,000 ≤1.5 Subclav/IJ Line ≥30,000 ≤1.5 Renal Biopsy ≥50,000 ≤1.5 Liver Biopsy ≥50,000 ≤1.5 Hickmann, Groshong Catheters ≥50,000 ≤1.5 *These numbers assume normal platelet function. Conditions that may affect platelet function include renal failure, medications, leukemias and myelodysplasias, and congenital disorders. Bleeding Time is a poor predictor of surgical bleeding. The Usefulness of Platelet Function Analysis (PFA) in predicting surgical bleeding is unknown.
study shows most ffp transfused is inappropriate (crit care med 2007;35:1655)
FFP can be thawed in warm running water in 5 minutes or microwave in 6 minutes with the same activity as waterbath (Anesth Analg 2006;103(4):969)
FFP can probably be refrozen (Transfusion 1989;29(7):600)
ABO Identical is better than compatible (Kenji Inaba Arch Surg 2010)
J Emerg Med. 2014 doi: 10.1016/j.jemermed.2014.04.042
Eighty-seven patients were entered into the study, and were administered a total of 199 units of FFP. Δ INR 1 unit FFP value was 0.03 ± 0.13 for patients whose pretransfusion INR level was under 2; 0.77 ± 0.47 for those between 2 and 5; 2.14 ± 0.63 for those between 5 and 9; 3.34 ± 0.89 for those between 9 and 12; and 4.63 ± 1.99 for those over 12. A very strong positive correlation was found between pretransfusion INR and Δ INR 1 unit FFP (p < 0.001, r = 0.957).
Cryoprecipitate
15 cc per unit
vWF, Hemophilia
cold precipitation and centrifugation of FFP
Concentrated factor VIII, vWF, fibrinogen, and factor XIII
Can also provide hemostasis in uremic patients possibly by reversal of qualitative platelet dysfunction.
Give 1 bag per 10 kg of body weight, this will increase fibrinogen 50 mg/dl
10 bags then 6-10 bags Q8
Transfuse if fibro level < 80-100 mg/dl
1 unit of FFP has twice the fibrinogen as 1 unit cryoprecipitate
Cryoprecipitate (CRYO) Description Cryoprecipitate is prepared from plasma and contains fibrinogen, von Willebrand factor, factor VIII, factor XIII and fibronectin. Cryoprecipitate is the only adequate fibrinogen concentrate available for intravenous use. Cryoprecipitate is available in pre-pooled concentrates of six units. Each unit from a separate donor is suspended in 15 mL plasma prior to pooling. For use in small children, up to 4 single units can be pooled. Each unit provides about 350 mg of fibrinogen. Indications for Cryoprecipitate Cryoprecipitate is indicated for bleeding or immediately prior to an invasive procedure in patients with significant hypofibrinogenemia (<100 mg/dL). Cryoprecipitate should not be used for patients with von Willebrand disease or Hemophilia A (Factor VIII deficiency) unless they do not (or are not known to) respond to DDAVP and recombinant and/or virally inactivated preparations are not available. It is not usually given for Factor XIII deficiency, as there are virus-inactivated concentrates of this protein available. Cryoprecipitate is sometimes useful if platelet dysfunction associated with renal failure does not respond to dialysis or DDAVP. Usage and Therapeutic Effect Cryoprecipitate – Dosage 1 bag contains ~350 mg Fibrinogen 6 bags (1pool) contains 2100 mg Fibrinogen Recovery with transfusion = 75% 6 bags cryoprecipitate provides 1560 mg Fibrinogen 70 kg X .05 = plasma volume of 35 dL (3.5 L) 1560 mg = 45 mg/dL provided by 6 bag pool of cryoprecipitate 35 dL In a 70 kg Patient: 6 bags (1pool) of cryo raises Fibrinogen 45 mg/dL Fibrinogen replacement: Effect can be monitored by fibrinogen level assay and clinical response. To replace factor VIII or von Willebrand factor: When specific factor concentrates are unavailable, the usual adult dose is a pool of 6 – 12 bags. Approximately 150 units of factor VIII and von Willebrand factor are provided per bag. A single donor may be used repeatedly for a young or mildly affected patient to limit donor exposures. Fibrin glue: Although single units of cryoprecipitate are available for use in the preparation of locally applied for surgery, commercially available, virally inactivated concentrates have a higher fibrinogen concentration and are preferred for this purpose (Tisseel®). A patient may donate autologous plasma for processing into cryoprecipitate prior to a planned surgical procedure. Do not use bovine, assoc with ATIII deficency
Albumin
25% is SPA, give 500cc saline c every 25 g
Platelets
50 cc per unit
Usual dose is 1 unit per 10 kg or 6 units (6 pack)
each unit raises plt by ~5000
Platelets are pooled at time of transfusion; they only last ~4 hours after pooling
5 pack of Platelets contains 1 unit of FFP
ABO compatibility is desired, but not essential
Platelets are essential for the initial phase of hemostasis. Platelet concentrates also contain about 60mL of plasma (coagulation factors) and small numbers of red blood cells and leukocytes. Platelet units must be maintained at room temperature and agitated during storage. Pooled random donor platelet concentrates are prepared from platelets that have been harvested by centrifuging units of whole blood. Up to 8 units of platelets, each from a separate donor, can be pooled into a single bag for transfusion. Platelets expire 4 hours after pooling. All units are from the same ABO type. If ABO compatible platelets are unavailable, ABO incompatible platelets can be substituted with very little risk. The usual adult dose is 4-6 units of pooled random donor platelets. Apheresis platelets, collected from a single donor, are prepared in standard (equivalent to ~4 pooled units) and large (equivalent to ~6 pooled units) sizes. An apheresis platelet concentrate contains 200-400mL of plasma. They may be collected as a random unit (random apheresis platelets) or be obtained for a specific recipient from a family member or a volunteer HLA compatible “directed” donor. Apheresis platelets expire 4 hours after processing for release from the blood center. Indications 1. To prevent bleeding due to thrombocytopenia. The threshold of thrombocytopenia at which bleeding may occur will vary depending on the patient’s clinical condition. In general, spontaneous bleeding does not occur until the platelet count falls below 5,000 – 10,000/µL. The recommended trigger for prophylactic platelet transfusions in patients undergoing chemotherapy or hematopoietic stem cell transplantation is <10,000/µL. 2. In a bleeding patient a platelet count above 50,000 should be maintained. In a surgical patient, the necessary platelet count varies depending on the procedure. For most surgeries 30,000-50,000/µL will be adequate. For high risk procedures, such as neurologic or ophthalmologic surgeries, 100,000/µL is recommended. 3. Abnormal platelet function may be congenital, or due to medications, sepsis, malignancy, tissue trauma, obstetrical complications, extra corporeal circulation, or organ failure such as liver or kidney disease. Spontaneous bleeding may then occur at higher platelet counts. If platelet dysfunction is present, the patient with a disrupted vascular system (e.g. trauma or surgery) will require a higher platelet count to achieve hemostasis. 4. Family donor or HLA matched platelets are indicated when patients have become refractory to random donor platelet transfusions due to alloimmunization. 5. In several situations platelet transfusions may not be indicated unless there is significant bleeding. In autoimmune thrombocytopenias (e.g. ITP) transfusion increments are usually poor and platelet survival is short. Platelet transfusions are contraindicated in patients with thrombotic thrombocytopenic purpura (TTP) unless there is clinically significant bleeding. Therapeutic Effect Expected Platelet Increment* 1 unit 1.0 x 1011 4 units 4.0 x 1011 6 units 6.0 x 1011 50 lb/23 kg 22,000/ul 88,000/ul 132,000/ul 100 lb/45 kg 11,000 45,000 66,000 150 lb/68 kg 7,400 30,000 44,000 200 lb/91 kg 5,500 22,000 33,000 *In a patient with a normal sized spleen and without platelet antibodies. The survival of transfused platelets averages 3 to 5 days but will decrease if a consumptive process is present. Correction of a prolonged bleeding time in platelet dysfunction will depend on whether a condition exists that will affect the transfused platelets as well (e.g., aspirin, uremia).
15 minute post-transfusion get a platelet count; if it drops instead of rises, consider HLA conflict
Factor VIIa
review article (Injury 2006;37:1172)
BEst Review to date (The American Surgeon 2008;74(12):1159)
May stop otherwise intractable bleeding, extremely expensive
At this stage the following recommendations can be made: 
 Where the use of Factor VIIa is being considered, hospitals should have a set of guidelines in place for the availability and use of Factor VIIa. The use of Factor VIIa should be closely monitored and ideally submitted to a national or international registry. Factor VIIa will not stop surgical haemorrhage. Factor VIIa should not be given instead of other blood product administration. Adequate FFP, Cryoprecipitate and Platelets need to be present for full effect. Factor VIIa should not be used too early, but neither should it be used only after ‘super-massive’ transfusions of 40-60 units. Therapy at between 8 and 20 red blood cell infusions is probably appropriate. (opinion only) The current recommended dose is 100micrograms/kg. This dose should be repeated at 1-2 hourly intervals if required. The Prothrombin time is used to monitor drug effect When the pH is below 7.2, consideration should be given to: increasing the dose of Factor VIIa Treating the patient with bicarbonate or THAM to raise the pH (Trauma.org)
Where the use of Factor VIIa is being considered, hospitals should have a set of guidelines in place for the availability and use of Factor VIIa. The use of Factor VIIa should be closely monitored and ideally submitted to a national or international registry. Factor VIIa will not stop surgical haemorrhage. Factor VIIa should not be given instead of other blood product administration. Adequate FFP, Cryoprecipitate and Platelets need to be present for full effect. Factor VIIa should not be used too early, but neither should it be used only after ‘super-massive’ transfusions of 40-60 units. Therapy at between 8 and 20 red blood cell infusions is probably appropriate. (opinion only) The current recommended dose is 100micrograms/kg. This dose should be repeated at 1-2 hourly intervals if required. The Prothrombin time is used to monitor drug effect When the pH is below 7.2, consideration should be given to: increasing the dose of Factor VIIa Treating the patient with bicarbonate or THAM to raise the pH (Trauma.org)
Review (Crit Care Med 2005; 33:883890))
VIIa is thought to act locally at the site of tissue injury and vascular wall disruption, by binding to exposed tissue factor and generating small amounts of thrombin that are sufficient to activate platelets.
The activated platelet surface can then form a template on which recombinant factor VIIa can directly or indirectly mediate further activation of coagulation, resulting in the generation of much more thrombin and, ultimately, fibrinogen to fibrin conversion (2, 3). Clot formation is stabilized by inhibition of fibrinolysis, due to factor VIIa-mediated activation of thrombin-activatable fibrinolysis inhibitor.
dose for trauma (40 mcg/kg)
need fibrinogen > 120 for it to work well
New parallel RCTS for blunt and penetrating (J Trauma 2005;59(1):8-18.
Evidence based Guidelines (J Throm Haemostasis 2005;3(3):640-8)
Indication Any salvageable patient suffering from massive, uncontrolled hemorrhage that fails to respond to appropriate surgical measures and blood component therapy. Definitions Massive bleeding is defined as one of the following [49,50]: Loss of entire blood volume within 24 h (10 U of packed RBC in a patient weighing 70 kg). Loss of 50% of blood volume within 3 h. Blood loss at a rate of 150 mL min1. Blood loss at a rate of 1.5 mL kg1 min1 for 20 min. Failure to arrest the hemorrhage despite: Application of all accepted and available surgical measures (e.g. ligation of damaged vessels, tamponading, or packing of the bleeding site, and induction of localized thrombosis). Appropriate replacement therapy: [5052]. FFP: 10-15 mL/kg (46 U for a patient weighing 70 kg). Cryoprecipitate: 12 U /10 kg (1015 U for a patient weighing 70 kg). Platelets: 12 U 10 kg (1015 U for a patient weighing 70 kg). Correction of acidosis (defined as pH 7.2). Warming of hypothermic patients (recommended, but not mandatory for administration of rFVIIa). Contraindications Absolute Unsalvageable patients, as identified according to the clinical evaluation of the treating medical team. Relative History of thromboembolic events (e.g. pulmonary emboli, myocardial infarction, cerebrovascular accident, deep vein thrombosis) within the previous 6 months. Administration guidelines for rFVIIa The blood bank should be immediately alerted to incidents of massive bleeding to facilitate timely preparation of the various blood components required [50]. rFVIIa should be administered as early as possible (after conventional treatments have failed to arrest bleeding), and should be given in conjunction with transfusion of 810 U of packed RBC in order to avoid further loss of clotting factors, exacerbation of acidosis, and further lowering of body temperature (all of which adversely affect the prognosis). Preconditions for rFVIIa administration Hematological parameters As rFVIIa acts on the patient’s own clotting mechanism, its administration should be considered after blood component therapy has achieved the following: Fibrinogen levels of 50 mg dL1 (preferably 100 mg dL1). Platelet levels of 50 000 109 L1 (preferably 100 000 109 L1). If these parameters cannot be monitored on an immediate basis (i.e., in ‘real time’ by point of care testing), as is usually the case, the patient should receive appropriate empirical replacement therapy (as previously defined). pHClinical and laboratory evidence suggests that the efficacy of rFVIIa decreases at a pH of 7.1 [15]. Hence, correction of the pH to 7.2 is recommended prior to its administration. Body temperature rFVIIa retains its activity in the presence of hypothermia, hence, the latter does not limit its use. Nonetheless, body temperature should be restored to physiological values as much as possible. Note: As laboratory tests are conducted at 37°C, they may not demonstrate the true measure of coagulopathy in a hypothermic patient. rFVIIa and surgical hemostasis It is recommended that rFVIIa be administered as an adjunctive therapy to concomitant surgical measures, as the agent arrests coagulopathic, rather than surgical, bleeding. If packing was performed, unpacking should be considered before administration of rFVIIa. This is recommended because the cessation of diffuse coagulopathic bleeding induced by rFVIIa and the hemodynamic improvement that follows may serve to expose surgical bleeding sites that could not be previously identified. For the same reason, if hemorrhage is encountered outside the operating room, angiography or a ‘second look’ should be considered (depending on the clinical circumstances) to rule out surgical bleeding. It is important to mention that there are cases where administration of rFVIIa alone, prior to, or even without surgical intervention, led to cessation or marked slow-down of the bleeding. Dosage The recommended initial dose of rFVIIa for treatment of massive bleeding is 120 (100140) g kg1 administered intravenously over 25 min. This is based on the experience in hemophilia patients and analysis of data of our trauma patients. Repeat dosage If hemorrhage persists beyond 15-20 min, following the first administration of rFVIIa, an additional dose of 100 g kg1 should be considered. If the response remains inadequate following a total dose of >200 g kg1, the preconditions for rFVIIa administration should be re-checked, if possible, and corrected as necessary before a third dose is considered. If this is not feasible, the empirical administration of FFP (1015 mL kg1 or 46 U for 70 kg), cryoprecipitate (12 U 10 kg1 or 1015 U for 70 kg), and platelets (12 U 10 kg1 or 1015 U for 70 kg) should be considered, and the pH and calcium should be checked and corrected. Only after these measures have been applied should a third dose of rFVIIa 100 g kg1 be administered. Monitoring Currently, there is no laboratory method for monitoring the effect of rFVIIa. The best available indicator of rFVIIa efficacy is the arrest of hemorrhage judged by visual evidence, hemodynamic stabilization and a reduced demand for blood components. The PT is expected to shorten, frequently below the normal expected range (as there is TF in the test tube), but this does not reflect efficacy. Rotation thromboelastography and thrombin generation are future candidate tests for evaluation of efficacy of rFVIIa.
Review article on its use in trauma (Critical Care 2005;9(Sup 5):S37
alternative dosing 200 mcg/kg followed by 100 mcg/kg at 1 hour followed by 100 mcg/kg at 3 hours
specifically who would benefit from this product is still unclear. Some of the testimonials are fantastic, but again non-controlled. J Trauma. 2005 Jul;59(1):8-15; discussion 15-8. Related Articles, Links Recombinant factor VIIa as adjunctive therapy for bleeding control in severely injured trauma patients: two parallel randomized, placebo-controlled, double-blind clinical trials. Boffard KD, Riou B, Warren B, Choong PI, Rizoli S, Rossaint R, Axelsen M, Kluger Y; NovoSeven Trauma Study Group. Department of Surgery, Johannesburg Hospital, University of the Witwatersrand, South Africa. kdboffard@pixie.co.za BACKGROUND: Uncontrolled bleeding is a leading cause of death in trauma. Two randomized, placebo-controlled, double-blind trials (one in blunt trauma and one in penetrating trauma) were conducted simultaneously to evaluate the efficacy and safety of recombinant factor VIIa (rFVIIa) as adjunctive therapy for control of bleeding in patients with severe blunt or penetrating trauma. METHODS: Severely bleeding trauma patients were randomized to rFVIIa (200, 100, and 100 microg/kg) or placebo in addition to standard treatment. The first dose followed transfusion of the eighth red blood cell (RBC) unit, with additional doses 1 and 3 hours later. The primary endpoint for bleeding control in patients alive at 48 hours was units of RBCs transfused within 48 hours of the first dose. RESULTS: Among 301 patients randomized, 143 blunt trauma patients and 134 penetrating trauma patients were eligible for analysis. In blunt trauma, RBC transfusion was significantly reduced with rFVIIa relative to placebo (estimated reduction of 2.6 RBC units, p = 0.02), and the need for massive transfusion (>20 units of RBCs) was reduced (14% vs. 33% of patients; p = 0.03). In penetrating trauma, similar analyses showed trends toward rFVIIa reducing RBC transfusion (estimated reduction of 1.0 RBC units, p = 0.10) and massive transfusion (7% vs. 19%; p = 0.08). Trends toward a reduction in mortality and critical complications were observed. Adverse events including thromboembolic events were evenly distributed between treatment groups. CONCLUSION: Recombinant FVIIa resulted in a significant reduction in RBC transfusion in severe blunt trauma. Similar trends were observed in penetrating trauma. The safety of rFVIIa was established in these trauma populations within the investigated dose range.
Recombinant Activated Factor VII for Acute Intracerebral Hemorrhage
Stephan A. Mayer, M.D., Nikolai C. Brun, M.D., Ph.D., Kamilla Begtrup, M.Sc.Joseph Broderick, M.D., Stephen Davis, M.D., Michael N. Diringer, M.D.,Brett E. Skolnick, Ph.D., and Thorsten Steiner, M.D., for the Recombinant Activated Factor VII Intracerebral Hemorrhage Trial Investigators*
From the Departments of Neurology and Neurosurgery, Columbia University College
of Physicians and Surgeons, New York (S.A.M.); Novo Nordisk, Bagsvaerd, Denmark
(N.C.B., K.B.); the University of Cincinnati
Medical Center, Cincinnati ( J.B.);
Royal Melbourne Hospital, University of
Melbourne, Melbourne, Australia (S.D.);
Washington University School of Medicine,
St. Louis (M.N.D.); Novo Nordisk, Princeton,
N.J. (B.E.S.); and the University of
Heidelberg, Heidelberg, Germany (T.S.).
Address reprint requests to Dr. Mayer at
the Neurological Institute, 710 W. 168th
St., Box 39, New York, NY 10032, or at
*The participating institutions and investigators
are listed in the Appendix.
N Engl J Med 2005;352:777-85.
Copyright © 2005 Massachusetts Medical Society.
background
Intracerebral hemorrhage is the least treatable form of stroke and is associated with
high mortality. Among patients who undergo computed tomography (CT) within three
hours after the onset of intracerebral hemorrhage, one third have an increase in the volume
of the hematoma related to subsequent bleeding. We sought to determine whether
recombinant activated factor VII (rFVIIa) can reduce hematoma growth after intracerebral
hemorrhage.
methods
We randomly assigned 399 patients with intracerebral hemorrhage diagnosed by CT
within three hours after onset to receive placebo (96 patients) or 40 ìg of rFVIIa per kilogram
of body weight (108 patients), 80 ìg per kilogram (92 patients), or 160 ìg per
kilogram (103 patients) within one hour after the baseline scan. The primary outcome
measure was the percent change in the volume of the intracerebral hemorrhage at 24
hours. Clinical outcomes were assessed at 90 days.
results
Hematoma volume increased more in the placebo group than in the rFVIIa groups. The
mean increase was 29 percent in the placebo group, as compared with 16 percent, 14
percent, and 11 percent in the groups given 40 ìg, 80 ìg, and 160 ìg of rFVIIa per kilogram,
respectively (P=0.01 for the comparison of the three rFVIIa groups with the
placebo group). Growth in the volume of intracerebral hemorrhage was reduced by
3.3 ml, 4.5 ml, and 5.8 ml in the three treatment groups, as compared with that in the
placebo group (P=0.01). Sixty-nine percent of placebo-treated patients died or were
severely disabled (as defined by a modified Rankin Scale score of 4 to 6), as compared
with 55 percent, 49 percent, and 54 percent of the patients who were given 40, 80, and
160 ìg of rFVIIa, respectively (P=0.004 for the comparison of the three rFVIIa groups
with the placebo group). Mortality at 90 days was 29 percent for patients who received
placebo, as compared with 18 percent in the three rFVIIa groups combined (P=0.02).
Serious thromboembolic adverse events, mainly myocardial or cerebral infarction, occurred
in 7 percent of rFVIIa-treated patients, as compared with 2 percent of those given
placebo (P=0.12).
conclusions
Treatment with rFVIIa within four hours after the onset of intracerebral hemorrhage limits
the growth of the hematoma, reduces mortality, and improves functional outcomes at
90 days, despite a small increase in the frequency of thromboembolic adverse events.
so it has value in even patients with normal coag panel
I write an annual essay on New Drugs and Devices for the educational website EMedHome.com, and then I develop a talk and slideshow which I take on the road. The year 2004 was kind of skimpy, but one item that caught my eye was the off-label uses and I must emphasize the off-label part for CME purposes of recombinant factor VIIa, commercial name NovoSeven, chemical name eptacog alpha activated. There was an article in the Wall Street Journal last March talking about this drug stopping bleeding in victims of gunshot wounds: now THAT got my attention. I practice in North Philadelphia, where on the July 4th 3 to 11 shift we saw eight people with gunshot wounds, three of whom were shot several times each. A systematic review of what we know so far was published in Critical Care Medicine 2005, Volume 33, pages 883 to 890. It was assembled and written by three physicians from the University of Amsterdam, and is entitled: Efficacy and Safety of Recombinant Factor VIIa for Treatment of Severe Bleeding. I guess what surprised me most is how little data is available only 1854 patients have been reported in 28 clinical trials, 124 case series, 176 case reports, and 155 other articles a total of 483 articles, but fewer than 4 patients per paper. Then 156 of those articles involving 408 patients were about hemophilia obviously this doesnt apply to our patient population. There were another 109 articles concerning coagulation disorders other than hemophilia, everything from thrombocytopenia to Factor XI deficiency. Now 37 of the articles discussed use of recombinant Factor VIIa in 684 patients with liver disease. A placebo-controlled trial in 245 patients with cirrhosis and portal hypertension who presented with upper GI bleed used a dose of 100 mcg/kg in addition to endoscopic and pharmacologic treatment. The number of patients with uncontrollable bleeding was reduced from 15.4% in the placebo group to 7.9% in the treatment group, although this effect was seen only in those patients with severe disease Childs category B & C. This is a good example of spectrum bias. Unfortunately, the data on trauma patients is still not ready for prime time, although several case reports and case series relate some tantalizing results. But remember that the plural of anecdote is not data. A large placebo-controlled trial using recombinant factor VIIa in 301 victims of severe blunt or penetrating trauma was just published in the Journal of Trauma July 2005 issue. In blunt trauma, packed red cell transfusion was significantly reduced with recombinant factor VIIa relative to placebo, with estimated reduction of 2.6 units, p value 0.02), and the need for massive transfusion defined as more than 20 units of blood, was reduced from 33% of patients to 14%, with a p value of 0.03. In penetrating trauma, the numbers werent nearly as good and never reached statistical significance. But transfusion is a surrogate marker, or a DOE data-oriented evidence rather than POEM patient-oriented evidence that matters. Trends toward a reduction in mortality death rate 25% in treated group vs. 30% in untreated – and critical complications acute respiratory distress syndrome (ARDS) and multiple organ dysfunction syndrome (MODS) – were observed. Adverse events including thromboembolic events were evenly distributed between treatment groups. Death, ARDS, and MODS are POEMs, but the study didnt reach statistical significance. What about patients taking warfarin who need to be reversed in a hurry is this stuff better than fresh frozen plasma? So far theres been no head-to-head comparison, but five case reports and ten case series claim complete reversal of elevated INRs in patients taking a vitamin K antagonist, allowing for safe performance of invasive procedures. Be aware though that recombinant factor VIIa lasts only for 2 or 3 hours, compared to 8 hours for other prothrombin complex concentrates. Finally, what about using it as a last-ditch effort in patients with life-threatening bleeding. There are no clinical trials that look at patients with excessive bleeding, but 21 case reports and 5 case series which made publication discuss using this drug for the rapid reduction of blood loss. Of course, there may also be hundreds reports filed away where the drugs did nothing, perhaps reflecting a publication bias. A recent New England Journal article caused a lot of excitement: 400 randomized patients with intracerebral hematoma were treated with varying doses of recombinant Factor VIIa . With all doses used, a repeat brain CT showed a smaller growth of the ball of blood than the nontreated group. Although this was a Phase II study in other words, looking for an effective dose the authors reported mortality figures as is now required by the FDA and it went from 29% in the placebo group to 18% in the treated group, a relative reduction of 35% and an absolute reduction os 11%, implying a number needed to treat of 9 to save one life. There was also an improved 90-day follow-up disability score in the treated group. Now those are POEMs rather than DOEs, but lots more work is going on in a recently started worldwide study. In addition, there was an increase in the number of patients who developed an ischemic stroke after being treated for their hemorrhagic stroke. Ive heard of a similar incident locally a patient admitted for intracerebral hemorrhage while taking warfarin, given 80 mcg/kg of recombinant factor VIIa and developing a dense hemiparesis from a new ischemic stroke. I also understand theres a lot of recombinant factor VIIa being used on injured American troops in the Gulf War Theater, and I anticipate gleaning valuable information from that data when it is published. Whats the downside?? Well, any clinical condition mediated by tissue factor exposure to the circulation can theoretically be made worse for instance a semi-ruptured atherosclerotic plaque which contains a large amount of tissue factor; that of course is the mechanism for an MI. Another example is DIC disseminated intravascular coagulation due to exposure of tissue factor on circulating mononuclear cells recombinant factor VIIa could thus aggravate systemic microvascular thrombosis in DIC. Recombinant Factor VIIa activity is reduced linearly with reduced temperature, retaining approximately 50% of its activity at temperatures of 28oC. However Factor VIIa activity on platelet surface membranes rises as temperature falls, probably due to increased stability of the protein at lower temperatures. Thus hypothermia should have little effect on FVIIa activity. Factor VIIa activity falls dramatically over the pH range 7.4 to 6.8, such that TF:VIIa activity is reduced to 50% of normal at pH 7.0 and activity of VIIa on platelet surfaces reduces even faster. Decreasing the pH of the reactions decreases the rate of FXa formation by the FVIIa/TF complex. Conclusion?? The website www.trauma.org makes the following recommendations: · Where the use of Factor VIIa is being considered, hospitals should have a set of guidelines in place for the availability and use of Factor VIIa. · The use of Factor VIIa should be closely monitored and ideally submitted to a national or international registry. · Factor VIIa will not stop surgical haemorrhage. · Factor VIIa should not be given instead of other blood product administration. Adequate FFP, Cryoprecipitate and Platelets need to be present for full effect. · Factor VIIa should not be used too early, but neither should it be used only after ‘super-massive’ transfusions of 40-60 units. Therapy at between 8 and 20 red blood cell infusions is probably appropriate. (opinion only) · The current recommended dose is 100micrograms/kg. This dose should be repeated at 1-2 hourly intervals if required. · The Prothrombin time is used to monitor drug effect · When the pH is below 7.2, consideration should be given to: not using FVIIa (futility), increasing the dose of FVIIa, or treating the patient with bicarbonate or THAM to raise the pH (no evidence to support this) The jury is still out, but there is a lot of chatter about this drug. The company that manufactures it, NovoNordisk, is being scrupulously careful in talking about it in the United States the FDA frown on companies that promote drugs for off-label uses. But the company is positioning itself for recognition in anticipation of FDA approval for many bleeding disorders. They had a booth at the Pennsylvania ACEP State Scientific Assembly this Spring and, although there was absolutely no material available about off-label uses, their display triptych featured a silhouette profile of a human head with a large splatter of bright red in the center. When I recently attended conferences in Buenos Aires and Nice France, NovoNordisk was unhindered by US FDA regulations and willingly talked about its off-label uses. There is much more work to be done, much data to be gathered before this very expensive drug it costs about $10,000 per dose becomes a familiar part of our armamentarium. I must emphasize again that what I have been discussing is the off-label use of recombinant factor VIIa, and that I have absolutely no financial relationship with NovoSeven or any other pharmaceutical company.
rVII a generates thrombin without the need of factor VIII cleavage…through direct activation of factor X…this thrombin burst quickly turns into fresh fibrin…this fibrin is quickly transformed in to fibrin degradation products by hyperfibrinolysis if no one cares about stopping hyperfibrinolysis… and fibrin degradation products in turn reactivate the coagulation cascade thorugh a positive feedback loop, amplifying even more the generalized factor consumption. Attention paid to the relative elevated factor VIII activity levels in many of these patients, because Factor VIII is an acute phase reactant, and is largely secreted when there is activation of inflammation and endothelial activation. In conditions where there is not enough fibrinogen, and factor X is being continuously depleted, by continuous activation, there is some lab and clinical evidence that r VII a performance is not the one we desire. Did I make myself CLEAR??? claudia
Inactivated FVII and the recombinant nematode anticoagulant protein c2(NAPc2) are under study. NAPc2 is a potent and specific inhibitor of the ternary complex between tissue factor/FVIIa and FXa, and directly acts against tissue factor activity, which is claimed to be the strongest ethiology for the DIC proccess. Let´s see the next publications on this issue. claudia
Claudia > rVII a can undergo consumption in an hyperfibrinolytic state like any other exogenously administered > factor contained in the cascade. I’ve been reading your comments on traumatic coagulopathy & TEG with interest – and we have talked about this offline before. I totally agree that TEG gives a more functional view of coagulation that the traditional PT & APTT do. BUT I think you are over-interpreting the TEG results. The definitive statements you make about hyperfibrinolysis etc are simply not so definitive. Coagulation, anticoagulation and fibrinolysis are not discrete events but occur simultaneously and indeed the pathways have multipleinteractions, such that they act as amplification and control loops on the central coagulation pathway. As soon as you generate thrombin you generate a fibrinolytic state. So you will get a hyperfibrinolytic state when you have massive thrombin production – as with massive trauma. BUT you will also get a hyperfibrinolytic state with moderate trauma and shock as thrombomodulin is presented and leads to TAFI activation and as aPC consumes PAI-1. These responses may be appropriate provide they lie within the body’s homeostatic mechanisms – ie. to preserve flow in the shocked state and prevent massive intravascular coagulation. Or they may be pathological if they exceed the fragility threshold of the coagulation system. The problem with the TEG results is that, as with PT and APTT, we really do not yet understand what we are measuring and hence what processes we are observing and hence what we should do about them. I think TEG is useful – but coagulation is nowhere near as clearcut as an ECG and the TEG is, ultimately, simply a measure of clot quality over time. And I disagree with your statement above. Fibrinolysis does not consume coagulation factors. Fibrinolysis may remove clot formed when there is massive activation of coagulation leading to their consumption, or there is systemic anticoagulation. tPA, uPA, plasmin, TAFI and PAI-1 do not act directly on the coagulation proteins. True, in a fibrinolytic state where PAI-1 is low, aPC will be dominant and anticoagulation ensue through inhibiton of factors V & VIII. But this is anticoagulation, not consumption – and the distinction is important because therapy could easily make things worse, not better. Karim
Reversal of warfarin induced excessive anticoag with factor vii (Ann Intern Med 2002;137:884)
Activated factor VII There was a minor flood of articles in 2005 dealing with a very hot topic in trauma care: the use of recombinant human activated factor VII (rFVIIa). rFVIIa was first introduced for clinical use in the mid 1980s, and the US Food and Drug Administration (FDA) approved its use in March, 1999, for patients with hemophilia A and B, especially those with inhibitors to factor VIII or factor IX. Since then, its use has undergone explosive growth in the United States and Europe, by far, mostly for ”off-label” indications. It has been described for trauma, cerebral bleeds, cirrhosis, gastrointestinal bleed, sepsis-induced disseminated intravascular coagulation (DIC), necrotizing pancreatitis, pulmonary alveolar hemor- The Literature of Emergency Medicine 525 rhage, and reversal of coumadin anticoagulation. For trauma, it is being used not only by trauma surgeons in the ED, OR, and ICU, but is being strongly considered for use by paramedics in the prehospital arena, as well as in rural areas and forward-deployed military units without access to blood bank or definitive surgery. The first use in a trauma patient was reported in Lancet in 1999; the first US trauma patient use was reported in 2002. Most reports of its use in surgical and trauma patients are dramatic. For example, the first US use in a trauma victim came after the patient had had 3 operations, 2 interventional angiographic procedures, and 105 U of PRBC, and was still bleeding at 45 hours after injury. A single dose (100 lg/kg) of rFVIIa stopped all bleeding immediately. The mechanism of action of rFVIIa is at least 3-fold. First, factor VIIa binds to exposed tissue factor at sites of endothelial injury to form factor Xactivating complex (as well as factor IXactivating complex); thus, clot formation is thought to be limited to the site of injury. Second, factor VIIa can also activate factor X on the surface of activated platelets even in the absence of tissue factor. Third, it also inhibits local fibrinolysis by activating thrombin-activatable fibrinolysis inhibitor. The dose for hemophilia is 90 lg/kg every 2 hours until hemostasis is achieved; for patients with trauma, most centers are using 90 to 120 lg/kg. Its half life is 2.3 hours, and a second dose can be given after 2 hours if needed. Its trade name is NovoSeven (Novo Nordisk, Inc). Its cost is huge: it comes in 1.2-mg ($731), 2.4-mg ($1427), and 4.8-mg ($2826) vials; a dose of 90 lg/kg for an 80-kg person thus costs about $4500. Here are the most important articles, all from 2005: Holcomb JB. Use of recombinant activated factor VII to treat the acquired coagulopathy of trauma. J Trauma 2005;58(June):1298-1303 [Commander USA ISR/Brooke]. This is the best review article. Get it and read it. Haan J, Scalea T. A Jehovah’s witness with complex abdominal trauma and coagulopathy: use of factor VII and a review of the literature. Am Surg 2005;71:414-415 [Maryland Shock Trauma]. This is a case report of a 23-year-old Jehovah’s witness patient with blunt splenic and left diaphragmatic injury, and left hepatic vein injury. The patient was coagulopathic and bleeding diffusely after surgical control. After a single dose (90 lg/kg) of FVIIa, the bleeding resolved almost immediately. Chino J, Paolini D, Tran A et al. Recombinant activated factor VII as an adjunct to packing for liver injury with hepatic venous disruption. Am Surg 2005;71:595-597 [UNM]. This report describes 2 children with blunt hepatic vein injury. A single 90 lg/kg dose caused rapid, dramatic cessation of coagulopathic bleeding. Benharash P, Bongard, F, Putnam B. Use of recombinant factor VIIa for adjunctive hemorrhage control in trauma and surgical patients. Am Surg 2005;71:776-780 [Harbor-UCLA]. This is a retrospective review of 15 patients (9 trauma, 5 cardiac or vascular, and 1 general surgical patients) who developed coagulopathy after major procedures, with massive bleeding despite surgical control. These patients were in dire straits: the mean international normalized ratio was 4.3; partial thromboplastin time (PTT), 125; temperature, 35.4 8C; base deficit, 5.2; and lactate, 8.9 mg/dL. The mean number of transfusions in 24 hours before the administration of factor VIIa was 17 U of PRBC, 8 fresh frozen plasma, 23 platelets, and 20 cryoprecipitate. Of the 15, 12 had partial or complete hemostatic response to 90 to 120 lg/kg (average initial dose, 7.3 mg); 3 patients received a second dose of 60 to 90 lg/kg. These 12, all of whom had been expected to die, stopped bleeding and lived at least 48 hours; 7 survived to hospital discharge. There were no thrombotic adverse effects. Levi M, Peters M, Buller HR. Efficacy and safety of recombinant factor VIIa for treatment of severe bleeding: a systematic review. Crit Care Med 2005;33(April):883-890. Levi et al reviewed all the literature for use of rFVIIa, finding 156 articles/408 patients on its use for hemophilia; 109 articles/242 patients, effective for a wide variety of platelet disorders; 37 articles/684 patients with liver disease, in which rFVIIa was quite effective for variceal bleeders, hepatectomy, and liver transplant; 47 articles/84 general surgery patients; and a randomized controlled trial (RCT) performed on patients undergoing prostatectomy, which found rFVIIa to be very effective. rFVIIa works for reversal of heparin anticoagulation therapy, but it only lasts 2 to 3 hours, vs 8 hours after prothrombin complex concentrates are used. rFVIIa also blocks/reverses the new pentasaccharide anticoagulants fondaparinux and idraparinux and, perhaps, even ximelagatran (a new direct thrombin inhibitor). The adverse effects were few: serious adverse events in all patients with hemophilia were less than 1%, and in all other patients, DVT occurred in 1.4%, probably many unrelated to the factor VIIa. Boffard KD, Riou B, Warren B et al. Recombinant factor VIIa as adjunctive therapy for bleeding control in severely injured trauma patients: two parallel randomized, placebo-controlled, double-blind clinical trials. J Trauma 2005;59(July):8-18. This is the most important article regarding the use of rFVIIa in patients with trauma. It was a multicenter (32 centers in 8 countriesSouth Africa, Israel, France, Germany, Canada, Australia, Singapore, UK) prospective double-blinded RCT. It was actually 2 simultaneous double-blinded RCT: 1 with 143 patients with blunt trauma, and 1 with 134 patients with penetrating trauma. In both, patients were between the ages of 16 and 65 years; exclusions included those in cardiopulmonary arrest, those with gun shot wound of the head or with a pH lower than 7.0, or an injury more than 12 hours old. Of interest, informed consent was waivedthis study could not be done in the United States. Patients were randomized after requiring 6 U of PRBC in the first 4 hours. The first dose of rFVIIa was 200 lg/kg, followed by 100 lg/kg 1 hour later, and 100 lg/kg in another 2 hours. The findings included a significant reduction in the number of transfusions and a trend to decreased mortality and critical complications (sepsis, adult respiratory distress syndrome, MODS). Again, adverse events were few: thromboembolism in 3% to 5% (total of 12: 6 in rFVIIa patients and 6 in placebo patients). Stein DM, Dutton RP, O’Connor J, et al. Determinants of futility of administration of recombinant factor VIIa in trauma. J Trauma 2005;59(Sept):609-615 [Maryland Shock Trauma Center]. This is a retrospective review from the years 2001 to 2003: of 81 patients at Maryland Shock Trauma Center who received rFVIIa, this article studied the 46 who were given rFVIIa for acute hemorrhagic shock within the first 4 hours. The dose was 100 lg/kg; the average number of units before giving rFVIIa was 25 (!!). Twenty-six patients responded with clinical resolution, only 2 requiring a second dose. Twenty patients did not respond, kept bleeding, and went on to die of hemorrhagic shock. Independent predictors of nonresponse were a higher serum lactate (12 vs 7), higher prothrombin time (PT) (21 vs 15) at the time of administration, and lower revised trauma score (4 vs 6) at the time of admission. Number of units transfused was not a predictor. MacLaren R, Weber LA, Brake H et al. A multicenter assessment of recombinant factor VIIa off-label usage: clinical experiences and associated outcomes. Transfusion 2005;45:1434-1442. These authors reviewed all 701 patients getting rFVIIa at 21 US academic medical centers during the 28-month period (January 2002 through May 04). Ninety-two percent were treated with the drug for an offlabel use: 38% to prevent bleeding in coagulopathic patients, and 62% to treat bleeding: surgical in 37%, gastrointestinal in 30%, intracerebral 526 The Literature of Emergency Medicine hemorrhage in 13%, and pulmonary in 10%. Two thirds received a single dose, a median of 75 lg/kg when used for prevention and 90 l g/kg when used for bleeding. Of note, the PT and international normalized ratio were always found to normalize after rFVIIa, whereas the activated PTT did not. In the prevention group, 14% bled, 5 of which were major bleeds. In the bleeding group, 53% stopped bleeding within 6 hours, but 25% rebled within 48 hours. Arterial pH below 7.2 was the only predictor of lack of response to rFVIIa. There was a 10% incidence of adverse events within 24 hours: 8 VTE, 3 myocardial infarction (MI), 3 DIC, 2 cerebrovascular accident (CVA), possibly although not definitely related to the rFVIIa. O’Connell KA, Wood JJ, Wise RP et al. Thromboembolic adverse events after use of recombinant human coagulation factor VIIa. JAMA 2006;295:293-298 [FDA]. This report comes from the FDA’s Adverse Event Reporting System (”MedWatch”), reviewing all AE’s between licensure of rFVIIa in March 1999 and the end of 2004, both from US and foreign/overseas hospitals. Of note, the authors state that the number of Adverse Event Reporting System reports usually significantly underestimates the actual number of occurrences. The authors found 168 reports describing 185 thromboembolic events; 151 of these were from use for off-label indications. Of the 185 thromboembolic events, 39 were embolic CVA, 34 were acute MI, 26 were other arterial thrombosis, 32 were pulmonary embolism, and 42 were DVT. Half of the adverse events occurred in the first 24 hours after drug administration. Of the 50 reported deaths, 36 were due to the thromboembolic event. The following is a summary of where we are vis-a`-vis rFVIIa: 1. rFVIIa is an exciting new agent for use in coagulopathic bleeding patients 2. It is extremely expensive, and its use at present is restricted to ongoing clinical trials The following are some of the main questions: 1. What is the optimal dose for the various indications? 2. Should it be used only for patients who are coagulopathic? And coagulopathic by what criteria? 3. When should it be used in actively bleeding patients? – Too early-wasted money, possible side-effects – Too late-the horse is out of the barn 4. There is ongoing concern about causing diffuse systemic microthrombi, causing not only DVT/pulmonary embolism, CVAs, MIs, and others but also later MODS 5. Laboratory studies/future directions
Since the first use of rFVIIa for the management of massive haemorrhage without underlying bleeding disorders, additional research has led to more understanding of its compartmentalised mode of action and contraindications concerning hypercoagulopathy have proved minimal. Recombinant FVIIa has become an established adjunctive therapy for the control of haemorrhage in severe trauma.2 Timing and conditions of rFVIIa administration are of great importance; administration too early, when bleeding still necessitates surgical intervention, may render the desired effect less likely. Other variables that should be taken into account are pH below 7.2 and core temperature below 35°.15 Of these, it is the pH that mainly affects the activity of rFVIIa. Martinowitz suggested pH correction first if lower than 7.2, with body temperature restored to physiological values as much as possible (despite minimal effect on efficacy of rFVIIa), and then administration of rFVIIa early, concomitantly with surgical measures.13 In all our cases the temperature threshold criteria were met, and the pH threshold was also met in cases 1 and 2 but not, at the time of the initial dose, in case 3. In the first 2 cases, coagulation parameters did improve after the initial administration of rFVIIa. In case 1, a second dose was added as venous oozing persisted, resulting in further improvement of coagulation. In case 3, no improvement in coagulation was seen following the first dose, with persisting haemorrhage even after 3 doses. In addition to a breached retroperitoneum above and below, the wound surface was probably too large to expect rFVIIa to be effective. The inability of the initial and subsequent doses to improve coagulation appears to confirm the hypothesis that, following an unsuccessful initial dose, the prognosis of additional rFVIIa is poorer.
Safety of VIIa-sig. increase in arterial but not venous thrombosis (NEJM 2010;363:1791)
Phase 3 trial of Factor VIIa
Journal of Trauma-Injury Infection & Critical Care: September 2010 – Volume 69 – Issue 3 – pp 489-500
no benefit
Dutton Safety Analysis of CONTROL Study
(J Trauma 2011;71:12)
increased MIs, no mortality benefit
Review of use shows what we all know–there is a dramatic and instant reduction in bleeding, this study couldn’t answer the long-term survival question (Acta Anaesthesiologica Scandinavica Volume 56, Issue 5, pages 636–644, May 2012)
Reactions
Acute
Acute Hemolysis
from ABO incompatibility, recipient complement destroys transfused cells
inflammatory response, hypotension, and vascular collapse.
DIC, renal failure
Patients will have fever with or without chills
fever, shock, flank pain, hematuriapink plasma in spun crit tubepositive coombs
Anaphylaxis
Microbial Contamination
staph, strep, yersenia
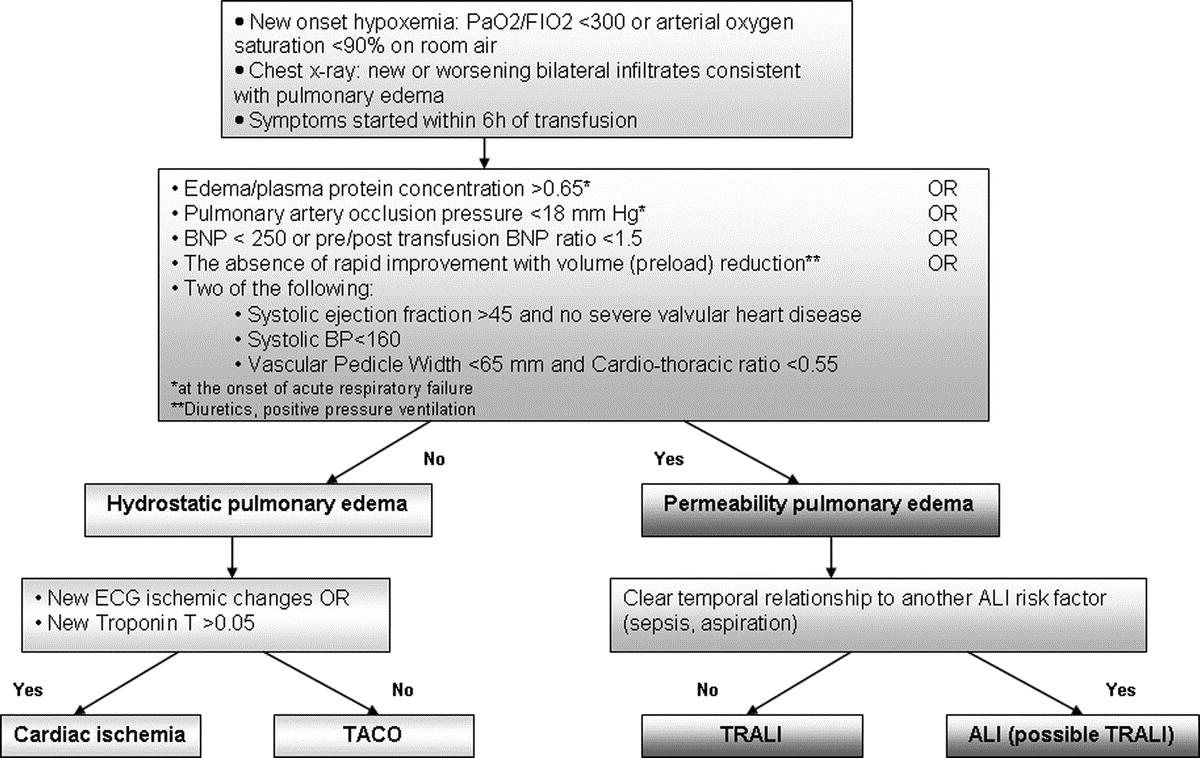
Noncardiogenic Pulmonary Edema
aka transfusion-related acute lung injury (TRALI)
Volume Overload
![]() What to do when their is a transfusion rxn
What to do when their is a transfusion rxn
minor reactions
feverrash (s fever)
Delayed
Infectious
HIV: 1 in 650,000
Hep C: 1 in 150,000
Hep B: 1 in 200,000
CMV
give cmv safe blood in seronegative pregnant women and negative recipients of organs
Effects of Massive Transfusion
Hypocalcemia-from citrate preservative
![]()
The busiest centers get the oldest blood. The way it works is the places which use blood least get the newest blood. When it is about to expire, it is transferred to the busy centers so it gets used up.
Tricc study and others show transfusion to 10 is not a better stategy than transfuse <7.
Transfusion Related Lung Injury (Trali)
Looney MR, Gropper MA, Matthay MA. Transfusion-related acute lung injury, a review. Chest 2004; July; 126:249-258
or Crit Care Med 2005;33(4):721
Review of Subject Crit Care Medicine 2006 May Supplement
BLOOD THERAPYAndrew Gettinger, MD, Associate Professor of Anesthesiology, Dartmouth Medical School, Dartmouth Hitchcock Medical Center, Lebanon, New Hampshire Introduction: 14 million units of allogeneic blood collected yearly in United States; approximately 12 million units of blood transfused; 3 to 4 million patients receive blood; between OR and ICU, anesthesia providers transfuse two thirds of blood supply; shortages real and increasing; donations decreasing; aging population increases demand on blood products and decreases likelihood of donation; blood progressively more expensive (acquisition costs have risen from $75-100 per unit to $250-300 per unit; addition of mandatory testing and processing raises price to $400-500 per unit) Risks associated with allogeneic blood: infections include HIV (1 in 900,000), hepatitis C (1 in 1.6 million), hepatitis B (1 in 180,000), and West Nile virus (extremely small risk); other risks include acute lung injury (1 in 5000), fatal hemolytic reaction (due to clerical error; twice as common as HIV transmission), immune suppression, and cancer recurrence; shelf life important Strategies to improve blood safety: 1) screening tests, 2) donor deferral, and 3) pathogen reduction technology Transfusion-related acute lung injury (TRALI): underrecognized; symptoms include respiratory distress, hypoxemia, hypotension, and fever; manifests 4 to 6 hr after receiving blood products; third most commonly reported category of fatalities associated with transfusion reported to Food and Drug Administration (FDA) Transfusion-induced immunosuppression: in early days of kidney transplantation, allogeneic blood used to increase allograft survival of transplanted kidneys by decreasing host immune response; animal studies show increase in tumor recurrence by impairing immune system; these effects thought due to leukocytes carried with red blood cells (RBCs); study in patients undergoing surgery for colorectal cancer indicates higher risk of developing infection with increasing blood transfusions (risk plateaus at approximately 20 units) Shelf life of blood: over time, pH progressively decreases, potassium progressively increases, and 2,3-diphosphoglycerate (2,3-DPG) and adenosine triphosphate (ATP) dramatically decrease; one study cited no improvement in tissue O2 consumption (VO 2 ) if blood stored >15 days; another study looking at tissue perfusion in gut found gastric tonometry decreased proportionally to age of blood (always decreased if blood >15 days old); rat model found VO 2 increased with fresh but not old RBCs Benefits of allogeneic blood: allogeneic blood has never been safer; anemia well documented as tolerated in healthy patients; alternative strategies continue to emerge (eg, hemodilution, more conservative treatment thresholds, pharmacologic alternatives); one study showed hemodilution well tolerated down to hemoglobin (Hb) 5 g/dL; subsequent study found cognitive changes associated with Hb <7 g/dL; follow-up study showed cognitive changes reversed with supplemental O2 ; study using careful acute normovolemic hemodilution demonstrated decrease in percentage of patients receiving allogeneic blood; another study found that with more conservative transfusion trigger, 33% of patients did not require transfusion and total number of transfusions reduced by 54%; results from 2 large observational cohort studies indicate pretransfusion Hb approximately 8.5 g/dL several years later; speaker suggests patient with unstable coronary syndrome be transfused and then followed closely (transfusion may make no difference immediately) Epoetin (EPO) critical care trials group: large study of 1300 critically ill patients randomized to EPO or placebo; summary indicates weekly dose of EPO results in significant decrease in patients who received transfusion; EPO treatment associated with decrease in cumulative RBC transfusions (20% reduction overall in allogeneic blood use); despite receiving fewer units of blood, patients who received EPO had higher Hb levels; no increase in mortality or morbidity as measured by adverse events; concluded that EPO given to critically ill patients can reduce exposure to allogeneic blood and raise Hb levels; additional study required to evaluate benefits Summary: transfusion decisions in ICU and OR not context mediated (ie, based on individual circumstances); patient with coexisting disease poses particular problem; for patient with preserved RBC mass, adequate time available to start interventions that deal with loss of RBC mass (especially one occurring over time in ICU) Use of leukocyte-filtered blood products: European blood banking community ahead of United States in mandating leukocyte-reduction technology and requirements; Canadians also have employed leukocyte-reduction program; 2 ways to leukocyte reduce allogeneic blood, either in blood bank (costly; 10% loss of blood product) or at bedside (easy to misuse) Clinical alternatives to hematocrit for measuring RBC mass:absolutely necessary; acute Hb and hematocrit [not] the right measure to make the decision
cohort study performed using data from nearly 79,000 patients enrolled in the Cooperative Cardiovascular Project (CCP) (36). The purpose of this study was to assess outcome in anemic patients, over age 65, with acute myocardial infarctions and the effect of blood transfusions in this group. Patients with a hematocrit of 27% or less who did not receive a transfusion had a 30-day mortality approaching 50% (11). Those individuals who had a hematocrit of less than 33% on admission and received a transfusion had a statistically significant lower mortality rate than those not transfused (36). PRBCs were shown to be harmful if administered to those with hematocrits over 36.1%. Although an observational study, this is the best evidence to date supporting a therapeutic hematocrit range of 33-36.1% in elderly patients presenting with acute myocardial infarction.
Component
Definition & Rationale
Clinical Scenario
Leukocyte-depleted
Contains less than 5 x 108 leukocytes.
- Prevent nonhemolytic febrile transfusion reactions
- Reduce rate of alloimmunization
- Reduce rate of leukocyte-associated viruses*
- Prevent transfusion-mediated immunosuppression (controversial)
- Hemoglobinopathies (Sickle Cell Disease, Thalassemias)
- Bone marrow or stem cell transplantation or potential for such transplantation in patients with solid tumor or hematologic malignancies
- Acute or chronic leukemia
- Congenital immune deficiency syndrome
Washed red cells
Suspended in saline after repeated saline washes to remove more plasma proteins and, to a lesser extent, leukocytes than was done from the originally donated whole blood.
Washes can be done to remove specific proteins.
Shelf-life of only 24 hours.
- Prevent anaphylactic reactions to plasma proteins
- Congenital IgA deficiency
- Patient with known allergy to leukocyte-depleted red cells
- Paroxysmal nocturnal hemoglobinuria
Irradiated
Gamma-irradiation to prevent donor lymphocyte proliferation.
- Prevent transfusion-associated graft-versus-host disease
- Hodgkins disease
- Congenital immune deficiencies affecting T-cells
- Wiskott-Aldrich syndrome
- Severe combined immunodeficiency
- Exchange transfusions in neonates
- Allogenic or autologous bone marrow transplantation
Frozen red cells
Frozen red cells in a glycerol solution that can be stored for up to 10 years; once thawed, must be used within 24 hours
- Maintain supply of rare blood donor phenotypes
- Patients with rare blood phenotypes who have developed alloantibodies
- Severe aplastic anemia in whom a transfusion cannot be avoided
CMV-negative
Prevent transmission of cytomegalovirus disease
- All pregnant women
- Intrauterine transfusions
- Neonates < 1200g born to CMV-negative mothers
- Infants under the age of 1 year-old
- CMV-negative AIDS patients
- HIV+ only: controversial
- CMV-negative bone marrow recipients or potential recipients
- CMV-negative solid organ transplant recipients
FFP Dose The dose is quite dependent upon the disorder being treated and the overall goal. There is approximately 1 unit/mL of activity of each coagulation factor per mL of FFP (7). A protime level greater than 1.5 times control equates to factor levels nearly 15% below normal (14). A mere increase of 2-3% of the coagulation factors is expected per transfused unit of FFP, assuming a normal level of factor production by the liver. Thus, to correct this factor level deficit of 15%, expect to transfuse at least 5 units of FFP (~3% per unit increase to correct the protime elevation of 1.5). Most of the time, this strategy is too cumbersome to perform. Therefore, the dose can be more easily estimated as 8-10mL/kg and can be ordered in units with each unit containing 200-250mL, irrespective of protime level (30).
Factor VII Recently, recombinant factor VIIa (rFVIIa) has shown efficacy in the treatment of hemophiliacs with factor inhibitors (12,15). These inhibitors are likely due to large genetic mutations that create alloantibody formation which inhibits the activity of factor replacements (16). Although the mechanism is not yet fully understood in vivo, rFVIIa combines with tissue factor to induce hemostasis independently of FVIII and FIX that eventually results in clot formation (29,38). Factor VIIa is a promising treatment modality for coagulopathic patients with defective thrombin production such as those with severe traumatic bleeding, complications from warfarin toxicity, or liver failure with gastrointestinal hemorrhage. Most evidence surrounding the use of rFVIIa in coagulopathic patients stems from observational case reports only. Post-partum hemorrhage in 3 patients requiring between 14-44 units of PRBCs was successfully halted with the use of rFVIIa (31). Similarly, 7 Israeli trauma patients, each receiving at least 20 units of PRBCs, were given rFVIIa based on compassionate use (21). In all 7 patients, the bleeding was said to have dried out within 15 minutes of administration, thereby greatly decreasing the PRBC requirement. Three of these patients died with the cause attributed to either sepsis or profound shock. Another case report series demonstrated normalization of the protime levels in coagulopathic neurosurgical patients prior to surgery for intracerebral hemorrhage (25). The cause of the coagulopathy in these patients ranged from warfarin toxicity to liver failure to severe trauma. Finally, there is a randomized controlled trial in swine demonstrating a significant decrease in bleeding from liver injuries due to rVIIa (12). Recently, rFVIIa has also been studied for use in patients without coagulopathy anticipated to have significant surgical bleeding from the procedure. A double-blind, placebo-controlled randomized study in patients undergoing retropubic prostatectomy (often associated with major blood loss and need for transfusion) found those who received rFVIIa to have less median blood loss than placebo (10). The cost of this medication – approximately $1500 per vial – may be justifiable in some circumstances.
Blood Component Modification
Recommendations
CMV Neg.1,2 Irradiation3 Leukocyte ReducedBM/Stem Cell Transplant Candidate X 4 5 Organ Transplant Candidate X Candidates for heart and kidney transplant. Chemo Rx Only 6 7 AIDS/HIV+ X Febrile Rxn’s 8 X Neonate X X Any Lymphopro- liferative Malignancy X
1. For patients with negative or unknown CMV serology.
2. Leukocyte depletion may be used if CMV negative blood components are not available.
3. All components for stem cell transplant patients require irradiation. All directed donations from family members or HLA matched donors require gamma irradiation.
4. Gamma irradiation is required pre-transplant for patients who may receive non-myeloablative (“mini”) transplants.
5. Required to prevent alloimmunization pre-transplant only.
6. Irradiation may be indicated in severely immunosuppressive chemotherapy, such as is used to treat patients with acute leukemia.
7. Leukocyte reduced blood is recommended for patients who will undergo multiple cycles of chemotherapy that will require platelet transfusion support.
8. If uncontrolled by leukocyte depletion, volume depletion of platelets prior to transfusion may decrease febrile reactions.
CMV NegativeCMV negative patients who are, or will be, severely immunosuppressed due to transplantation should receive only CMV negative platelets, whole blood and red blood cells to prevent primary CMV infection.
Premature infants and low birth weight neonates should receive CMV negative blood components regardless of serology.
Leukocyte depletion of blood is equivalent to CMV screening but is more expensive and indicated only if CMV negative blood is not available.
Irradiation (gamma)Inactivation of lymphocytes prevents transfusion induced GVHD due to engraftment of donor cells in an immunosuppressed patient.
Leukocyte-reduction (“leukopoor”)Removal of leukocytes by filtration of platelets and red blood cell concentrates is indicated for febrile transfusion reactions and when CMV negative components are indicated but not available.
Leukocyte depletion my prevent alloimmunization to platelets and should be used in patients who are expected to need platelet transfusions during multiple courses of chemotherapy and do not have pre-existing HLA antibodies.
Volume Reduced PlateletsRemoval of excess donor plasma is indicated in patients who cannot tolerate the full volume or when ABO incompatible single donor platelets are transfused. Volume reduction may be helpful in patients with febrile transfusion reactions that persist despite leukocyte reduction. Approximately 10% of the platelets are lost in this process and the extra centrifugation step may cause some platelet activatioin and loss of function.
Washed Red Blood Cells and PlateletsPatients with severe life threatening plasma allergies uncontrolled by medications or volume reduction may require red blood cells or platelets to be resuspended in saline. Washed red blood cells must be transfused within 24 hours or be wasted. The recovery and function of platelets after washing are severely impaired.
Blood Substitutes
Review of Blood Substitutes (Shock 2005;24(3):197-205)
Blood Bank Tests
![]()
![]()
![]()
![]()
(CMAJ 2006;174(1):29)
Rh antibody is not naturally occuring, it is created only after exposure to positive blood in a negative patient
Key Anti-RBC Antibodies
Kell (K), Duffy (Fy), Kidd (Jk), and Rhesus (Rh)
ABO compatability for plts is desirable but not necessary
cryoprecipitate does not require typing
Male RhoGAM
If a male Rh- gets O+, perhaps they should get rhogam (Journal of Trauma and Acute Care Surgery Volume 72(1), January 2012, p 48–53)