Guidelines for Management of Acute Liver Failure/Fulminant Hepatic Failure
by M. Njoku, MD
Dept of Anesthesia
University of Maryland Medical System
Criteria for definition
1)rapid development of hepatocellular dysfunction(ex. jaundice, coagulopathy)
2)encephalopathy within 8 weeks of onset of jaundice
3)absence of prior history of liver disease
Causes
Drugs are the most common cause
Acetominophen, halothane, isoniazid, valproate, sulfonamides, phenytoin,
Thiazolidinediones, herbal remedies
Hepatotropic viruses
Hepatitis Arare, usually good prognosis
Hepatitis Bmost common viral cause
Hepatitis Crare cause in Western countries
Hepatitis Drequires co-infection with HBV
Hepatitis Erare
Togavirus, transfusion transmitted virus, parvovirus B19
Unknown Etiololgy/Cryptogenic
Defined by negative serologic testing for HAV, HBV and absence of other known causes
Uncommon Causes
Wilsons disease
Other infections–EBV, herpesviruses, tuberculosis
Vascular abnormalitiesBudd Chiari syndrome, hepatic veno-occlusive
Disease
ToxinsAmanita phalloides ingestion, sea anemone sting, carbon
tetrachloride
Fatty liver of pregnancy
Autoimmune hepatitis
Malignant infiltrationlymphoma, melanoma, breast cancer
Ischemiahypotension, heat stroke
Reyes syndrome
Primary graft non-function following liver transplantation
Clinical Presentation
Nonspecific complaintsnausea, vomiting, fatigue, malaise, followed by
Jaundice
Complications of ALF
Encephalophathy
Stage 1change in affect, insomnia, difficulty with concentration
Stage 2drowsiness, disorientation, confusion
Stage 3marked somnolence, incoherence
Stage 4frank coma
Seizures
Cerebral edemaassociated with stage 3 and stage 4 encephalopathy
Hypoglycemia
CoagulopathyGI bleed, mucosal sites, vascular puncture sites
INR and PT correlate with severity of liver
Infectionimpaired immune function, nosocomial sources
Multiple organ failure syndrome
Management and Workup
Attempt to identify the cause
History, Physical exam
Toxicology Screen
Viral serology
Hep A IgM Ab, Hep A(IgG IgM) Anti-HAV, Hep B surface Ab, Hep B surface Ab quant, Hep B surface Ag, Hep C Ab screen, Hep C PCR, HSV IgG, HSV IgM, EBV IgG, EBV IgM, Rubella IgG screen, Varicella IgG
Rapid Tests
Hep A IgM Ab, HepBsurface Ag, Hep Bcore IgM Ab, HIV, CMV IgM,
CMV IgG
Autoimmune serology
Anti-nuclear antibody and titer, Ribonucleic protein antibody, Smith antibody, smooth muscle antibody, SS-A(Ro) antibody, SS-B(La), antibodies to liver-kidney-microsome type 1
Other Lab Tests
Alpha-1 antitrypsin, ceruloplasmin, alpha feto protein, HIV-1/HIV-2,
CMV IgG, CMV IgM, TSH, HCG
RUQ Ultrasound to assess vessel patency
CT/MRI
Consider transjugular liver biopsy
Etiology-specific Treatment(if indicated)
Acetaminophen toxicityN-acetylcysteine
Herpes-induced fulminant hepatitisIV acyclovir
Fatty liver of pregnancyemergency delivery
Autoimmune hepatitisglucocorticoid
Amanita phalloides ingestionpenicillin and silibinin
Early evaluation of candidacy for liver transplantation and referral to a transplant center
Immediately Consult
Hepatologist
Liver Transplant Surgeon
Transplant Anesthesiologist
Intensive medical management until spontaneous recovery, hepatic regeneration or liver transplantation
Measure electrolytes, ionized calcium, magnesium, phosphorus, BUN, creatinine,
glucose, ammonia, arterial lactate, LFTs, PT, PTT, INR every 6 8 hours
Correct electrolytes
Coags are utilized to assess prognosisNo need to correct coags in a patient who
is not bleeding
If serum glucose < 70
administer glucose in IVF
consider D50 bolus, D5 ½ NS, D5NS or D10/D20 + a balanced salt solution titrate glucose solution for FS 70 80
continue to monitor fingerstick q 1 2 hours
Neuro Exam q 1 hour
Report any worsening of neuro exam, lateralizing signs, posturing, or
seizures to house officer and transplant team
No sedatives, analgesics, or neuroleptics because of effect on neuro exam
Look for other causes of alteration in neuro exam
Electrolytes, glucose, acid-base, ventilation, oxygenation, subclinical seizures
Head CT for any worsening of neuro exam
Evaluate for edema, mass lesion, hemorrhage, brain stem herniation
Anticipate Intubation for airway protection and mechanical ventilation for
stage 3 or 4 encephalopaty
ICP monitoringconsider for stage 3 encephalopathy, usually required
for stage 4 encephalopathy
Consult Neurosurgery for epidural pressure monitor or subdural(Camino) catheter
Correct coags for epidural pressure monitor placement
Monitor for volume overload, may need diuresis
Decrease in IV fluids to accommodate FFP load
Consider Factor VII, instead of FFP, if fluid overload
(requires pharmacy/physician approval)
Coordinate optimal time of coag correction with
neurosurgery and OR team
Repeat Head CT following epidural pressure monitor placement
Consider measurement CMR or JvO2 or TCD
Treatment of Intracranial Hypertension(ICP > 15)
Maintain CPP 60 100(CPP = MAP ICP)
If CPP is low and MAP is low
optimize volume status, then consider inotrope
If CPP is low and ICP is elevated
utilize measures below:
Head elevation > 20o 30o, midline position
Intubation, Mild Hyperventilation, Normoxia
Active cooling, if febrile
Mannitol, if renal function intact, 0.5 mg/kg
monitor serum osmolarity and serum sodium q6h
withold mannitol for serum Na > 150 and serum Osm >320
Barbiturates¯CBV, ¯ICP, treat and prevent seizures
Titrate barbs to ICP £ 15 and CPP 60 100
If seizures present use EEG to confirm suppression
NOTE: The mechanism of death is cerebral edema and herniation if there is no spontaneous recovery or transplant
Lactulose (po), 30 cc bid to qid, for 4 5 stools per day
or Metronidazole(po) 250 mg qid
Enteral Nutrition, 35 50kcal/kg/d + protein 1gm/kg/d
DVT prophylaxis/pneumatic compression stockings
Coagulopathy includes inability to synthesize protein C, protein S, ATIII and a pro-coagulant state
Vitamin K 10mg IV q day x 3 days, for suspected deficiency
Stress ulcer prophylaxis
Monitor for signs and treat bacterial or other nosocomial infection
Invasive monitoring(CVP or PAC and arterial line as indicated) to guide
intravascular volume replacement and hemodynamics
Renal dysfunction
Correct volume deficits, electrolytes, acid-base abnormalities
Discontinue nephrotoxic agents
Rule out obstructive uropathy, parenchymal renal disease, UTI
Check urine microscopy, urine electrolytes, calculate FENa
Bicarbonate or tromethamine to correct acid base abnormalities depending
On serum sodium
Consider CVVHD for ARF unresponsive to other medical measures
Indicated for uncontrolled acidosis, hyperkalemia, fluid overload, management of cerebral edema with concomitant renal failure
Respiratory Dysfunction
Aspiration risk with progressive obtundation
Nosocomial pulmonary infection risk is increased
ARDS is associated with ALF and FHF
Consider intubation for airway protection as neuro exam worsens
Consider intubation to facilitate pulmonary toilet and improve gas
exchange
Obtain baseline EKG, CXR
Tissue and blood type
Kings College Hospital Criteria for Liver Transplantation
Acetaminophen-Induced FHF
Arterial pH <7.3(irrespective of grade of encephalopathy)
OR
Presence of all 3 of the following:
PT >100secs(INR > 6.5)
Grade III – IV encephalopathy
Serum creatinine >3.4 mg/dL
Non-Acetaminophen-Induced FHF
PT > 100secs(INR > 6.5)(irrespective of grade of encephalopathy)
OR
Presence of any 3 of the following:
Age <10yrs or >40yrs
Non-A, non-B hepatitis, halothane, idiosyncratic drug reaction, Wilsons
disease
Serum bilirubin > 17.5 mg/dL
Jaundice to encephalopathy time of greater than 7 days
PT > 50secs(INR > 3.5)
Contraindications for Liver Transplantation
Extrahepatic malignancy
Uncontrolled extrahepatic sepsis
Irreversible brain injury caused by intracranial hemorrhage
Unresponsive cerebral edema,
CPP < 40 for 2 hours or more
Persistent ICP > 40 mm Hg
Advanced cardiopulmonary disease
Active substance abuse
References:
Yee HF, Lidofsky SD. Acute Liver Failure. In: Feldman: Sleisenger & Fordtrans Gastrointestinal and Liver Disease, 7th edition, Philadelphia: Elsevier Science; 2002:
567 1576.
Krasko A, Deshpande K, Bonvino S. Liver failure, transplantation, and critical care. Critical Care Clinics 2003 April Apr;19(2).
Sanyal AJ, Stravitz RT. Acute Liver Failure. In: Zakim D, Boyer T, editors. Hepatology: A Textbook of Liver Disease. Philadelphia: Elsevier Science: 2003: 445 496.
Wendon J, Williams R. Transplantation for Fulminant Hepatic Failure. In: Busuttil RW, Klintmalm GB, editors. Tranplantation of the Liver. Philadephia: Saunders: 1996: 93 100.
Appendix
N-Acetylcysteine
Confirm hepatotoxic ingestion
7.5 gm, adult
150 mg/kg, child
Measure blood level at least 4 hours following ingestion
Correlate level with acetaminophen toxicity nomogram
Treatment may be beneficial up to 36 hours following ingestion
If treatment indicated, use the following guidelines
N-Acetylcysteine(po)
140 mg/kg followed by 17 additional doses of 70mg/kg every 4h
N-Acetylcysteine(IV)
Loading dose
150 mg/kg in 200ml 5% dextrose, infused over 15 minutes,
Maintenance dose
50 mg/kg in 500ml of 5% dextrose, infused over 4 hours,
followed by
100 mg/kg in 1000ml of 5% dextrose infused over 16 hours
Treatment for Amanita phalloides poisoning
Penicillin G 1gram/kg/d or 1.8 million U/ kg/d IV
And
Silibinin 20- 50 mg/kg/d IV
Recombinant Factor VIIa
100 mcg/kg IV rounded to nearest vial size, single dose
t1/2 2.3 hours
measure PT, PTT 1 hour following dose
Prednisone, Single Drug Therapy for Autoimmune Hepatitis
60mg/day x 1week, then
40mg/day x 1week, then
30mg/day x 2weeks, then
20mg/day until end point(remission, treatment failure, incomplete response, or drug toxicity)
Pentobarbital
Administration guidelines attached
Acyclovir for HSV
5 10 mg/kg every 8 hours, for 7 10 days
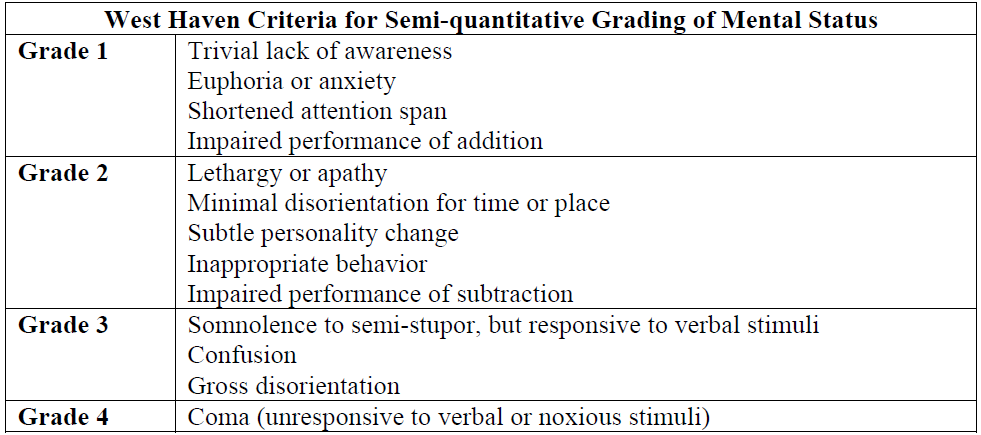
West Haven Criteria