Bad Bugs, No Drugs, No Escape
(CID 2009;49:992)
Enterococcus faecium
Staph Aureus
Clostridium Difficile
Acinetobacter baumannii
Pseudomonas aeruginosa
Enterobacteriaceae
Bacterialcidal vs. Bacteriostatic Probably Doesn’t Matter
J. Antimicrob. Chemother. (2015) 70 (2): 382-395.
Extended Spectrum Beta-Lactamases
E. Coli, Klebsiella, other Gram Neg Rods
Use Meropenem/Imipenem/Doripenem
Do not use cephalosporins of zosyn as the “inoculum effect” may ruin these drugs
Duration of treatment is the same
Carbapenem Resistant Gram Negative Rods (CREs)
Options for treating carbapenem-resistant Enterobacteriaceae
Retrospective and prospective (nonrandomized noncontrolled) studies provide data regarding the management of infections due to carbapenem-resistant Enterobacteriaceae. The combination of a carbapenem with colistin or high-dose tigecycline or aminoglycoside or even triple carbapenem-containing combinations if the minimum inhibitory concentration (MIC) range of carbapenem (meropenem and imipenem) resistance is 8 mg/l or less seems to have an advantage over monotherapy with either colistin or tigecycline or fosfomycin. For Enterobacteriaceae with MIC for carbapenems over 8 mg/l, combination regimens involve colistin, tigecycline usually administered in a double dose than that suggested by its manufacturer, fosfomycin and aminoglycosides in various combinations.
Summary: Suggestions based on the limited literature cannot be made safely. Combination regimens involving carbapenems for Enterobacteriaceae with MICs 8 mg/l or less for carbapenems (in dual combination with colistin or high-dose tigecycline or aminoglycoside or even triple combinations) seem to confer some therapeutic advantage over monotherapy. For Enterobacteriaceae with higher than the above-mentioned MICs, a combination of two or even three antibiotics among colistin, high-dose tigecycline, aminoglycoside and fosfomycin seems to confer decreased mortality.
Urinary Tract Infections
Signs and Symptoms
Pyuria with > 10 WBC per high-power field
Urine Cx > 100,000 organisms (stop empiric abx if cx negative)
—-
VRE: A Very Real Emergency Medicine Problem
With increasing prevalence of antimicrobial resistance among bacteria coupled with the lack of novel antimicrobial development, multi-drug resistant bacteria will continue to be problematic [1]. Due to this increased prevalence, it is likely that even in the emergency department, we will see more and more patients with prior cultures or past medical history documentation of multi-drug resistant bacteria, such as vancomycin resistant Enterococcus (VRE). Once we are aware of this information, how should this affect our decision making for treatment of these patients?
To help address this, assessment of the following clinical questions may be useful:
1) Is my patient likely to be ill from VRE?
Enterococcus is a common colonizing agent of the gastrointestinal tract and may also colonize the genitourinary tract as well as the skin [2]. As a result, care should be taken to determine colonization versus infection if VRE has been isolated.
In non-critically ill emergency medicine patients, examining for the presence of VRE risk factors may help to guide therapy. Some common risk factors include: [2]
- Recent administration of antibiotics (including but not limited to cephalosporins, clindamycin and metronidazole likely due to selective pressure for Enterococcus species)
- Recent or prolonged hospitalization or stay in a health care facility
- Compromised immune systems (hematologic malignancy, organ transplant)
- High severity of illness
In patients who are likely to be ill due to VRE, treatment should be started with an agent likely to be active against the VRE at the site of the infection.
2) How sick is my patient?
In critically ill patients with a past medical history positive for VRE, it is prudent to cover the patient for this organism until proven otherwise. There are no specific recommendations for VRE bacteremia in general; however, the 2009 clinical practice guidelines recommend either intravenous linezolid or daptomycin for the treatment of intravenous catheter-related bacteremia secondary to VRE [3].
3) Do I have culture data?
Past cultures isolated from previous infections may or may not be what is currently making the patient ill. For serious illness such as bacteremia or endocarditis, consideration of past culture data may be acceptable for select patients such as those who are sent in from an outside facility with recent culture data or a recent hospital visit where current cultures were obtained. For example, if a patient was seen last week with a urinary tract infection from VRE and is now presenting with symptoms of urosepsis, depending upon the clinical picture it may be reasonable to use the culture data from the prior week to base clinical decisions (see Table 1 below for treatment options).
For the more common infection of VRE cystitis, more treatment options may be available. Ideally, we will be able to choose the most narrow, tolerable, and cost-effective antimicrobial coverage for our patients.
Table 1: VRE Treatment Options [2-6]
| Infection Type | Ampicillin Sensitive VRE | Ampicillin Resistant VRE |
| Uncomplicated Urinary Tract Infections
(PO therapy only listed) |
– Ampicillin or Amoxicillin – Nitrofurantoin – Fosfomycin – Doxycycline |
– Nitrofurantoin – Fosfomycin – Doxycycline – Linezolid (if no other treatments are sensitive) |
| Complicated Urinary Tract Infections & Systemic VRE Infection | – Ampicillin + Aminoglycoside | – Daptomycin – Linezolid – Quinupristin-dalfopristin* |
*Limited activity against Enterococcus faecalis and poor patient tolerability
Table 2: Medication Dosing Regimens for VRE Based on Type and Source of Infection
| Indication | Medication | Dose‡ | Duration |
| Uncomplicated Urinary Tract Infections
(PO therapy only listed) |
Ampicillin | 250-500 mg PO q6 hours | 20-28 doses |
| Amoxicillin | 250-500 mg PO q8 hours | 15-21 doses | |
| Nitrofurantoin | 100 mg PO q12 hours¶ | 10 doses | |
| Fosfomycin | 3 g PO | 1 dose | |
| Doxycycline | 100 mg PO q12 hours | 10-14 doses | |
| Complicated Urinary Tract Infections & Systemic VRE Infection | Ampicillin
Gentamicin |
2 gm IV q4 hours
1 mg/kg IV q8 hours |
Duration depends upon location and severity of infection |
| Daptomycin | 8-12 mg/kg q24 hours | ||
| Linezolid | 600 mg IV/PO 12 hours | ||
| Quinupristin-dalfopristin | 7.5 mg/kg IV q8 hours |
Adapted from from Chambers HF, Elipoulos GM, Gilbert DN, Saags MS, eds. The Sanford Guide to Antimicrobial Therapy, 44th ed. Sperryville, VA: Antimicrobial Therapy; 2014.
‡Dosing for adult patients, not adjusted based on renal function
¶Dosing for Macrobid formulation
In conclusion, the “big gun” antibiotics of daptomycin or linezolid may not always be the go-to choice for VRE in the ED. Based on the suspected source of the infection and prior culture data when available, more narrow treatment with ampicillin or nitrofurantoin for example may be acceptable, easier to administer, and more cost-effective as treatment options in select patients.
References:
- Boucher HW, Talbot GH, Bradley JS, et al. Bad bugs, no drugs: No ESKAPE! An update from the Infectious Disease Society of America. Clin Infect Dis. 2009;48:1-12.
- Patel R, Gallaher JC. Vancomycin-resistant Enterococcal bacteremia pharmacotherapy. Ann Pharmacother. 2015;49(1):69-85.
- Mermel LA, Allon M, Bouza E, et al. Clinical practice guidelines for the diagnosis and management of intravenous catheter-related infection: 2009 update by the Infectious Disease Society of America. Clin Infect Dis. 2009;49:1-45.
- Baddour LM, Wilson WR, Bayer AS, et al. Infective endocarditis: Diagnosis, antimicrobial therapy, and management of complications: A statement for healthcare professionals from the Committee on Rheumatic Fever, Endocarditis and Kawasaki Disease, Council on Cardiovascular Disease in the Young, and Councils on Clinical Cardiology, Stroke, and Cardiovascular Surgery and Anesthesia, American Heart Association: Endorsed by the Infectious Disease Society of America. Circulation 2005;111:e394-e434.
- Heintz BH, Halilovic J, Christensen CL. Vancomycin-resistant Enterococcal urinary tract infections. Pharmacotherapy.2010;30(11):1136-49.
- Murray BE. Vancomycin-resistant Enterococcal infections. N Engl J Med. 2000;342(10):710-21.
Jill Logan, Pharm.D., BCPS (@EMPharm)
Emergency Medicine Clinical Pharmacist
Baltimore Washington Medical Center
Infections in the ICU
The Lancet, Volume 375, Issue 9713, Pages 463 – 474, 6 February 2010
Use of procalcitonin to reduce patients’ exposure to antibiotics in intensive care units (PRORATA trial): a multicentre randomised controlled trial
Treat cultures if in blood, in tissue, or 2 other sites simultaneously with signs of infection
CRP
acute phase proteins
Acute Phase ProteinsPositive Acute Phase Proteins: Proteins exhibiting increased plasma concentrations during the acute-phase response.
Factor VIII C reactive protein Ferritin Serum amyloid A Phospholipase A2 Haptoglobin a1 Alpha-1-protease inhibitor Ceruloplasmin C-1 esterase inhibitor Complement (C3 and C4) Mannose binding protein LPS binding protein
Prothrombin Plasminogen Immunoglobulins Plasminogen activator inhibitor-1 Alpha-1-acid glycoprotein Fibronectin Hemopexin Fibrinogen Pancreatic secretory trypsin inhibitor Inter-alpha protease inhibitor Alpha 2 macroglobulin C4b binding protein
Negative Acute Phase Proteins: Proteins exhibiting decreased plasma concentrations during the acute-phase response.
Albumin Transferrin Transthyretin (Pre-albumin) Alpha-2-HS glycoprotein
From Kushner I, Rzewnicki DL. The acute phase response. In: Mackowiak PA, ed. Fever, basic mechanisms and management, 2nd ed. Philadelphia: Lippincott-Raven; 1997:16576.
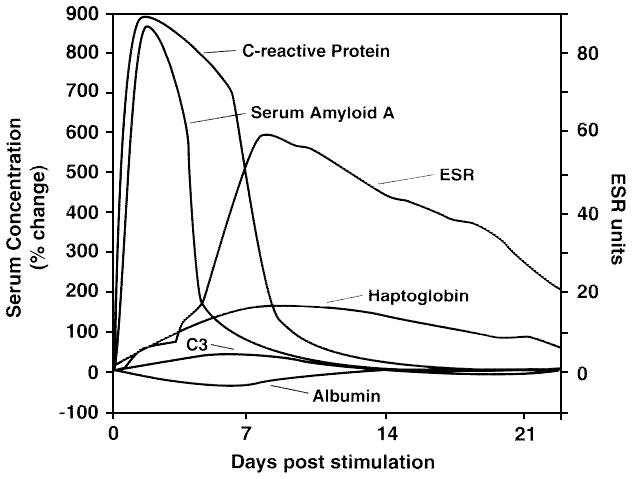
Table 6: Comparison of ESR and CRP (Ng. Br J Hosp Med 1998:58;521-523) [76]
Strep Pneumoniae
Risk Factors
Age>65
Beta Lactam within past 3 months
ETOH
Immunosuppression
Multiple medical comorbidities
Childcare or Daycare Exposure
MIC>2 mcg/cc is high level resisitance
also confers resistance to erythromyin, cipro,cepalosporins, tetracycline
VRE
treat c amp/genta as first line
Colonic bacteria
e. coli finds optimal conditions in the peritoneal cavity bacteroides also can survive
Sinusitis
always consider in all FUOs; very common in ventilated patients. (Critical Care 2005;9:R583)