Enteral Nutrition Myths by Paul Marik
Nutrition
Delay in enteral feeding causes impaired carb absorption in critically ill patients (Crit Care Med 2012;40:50)
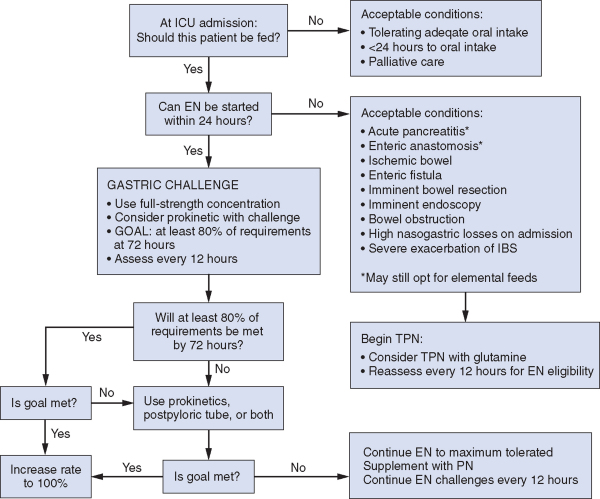
SCCM Guidelines (CCM Volume 37(5), May 2009, pp 1757-1761)
total water=60% body weight in males (40% IC 20% EC (5 % Plasma) and 50% in females (30/20) insensible/sensible losses=2000 to 2500 cc/day 3rd space/small intestine-LR colon/gastric-D5 1/2 with 30 KCl Nutrition 1/2 life of prealbumin=2-3 days measure CRP at the same time b/c prealbumin is a neg acute phase reactant, so may appear falely lowered despite adequate nutrition give 50% carb, 30% fat, 20% protein protein is 1.2-1.5 gm/day 1.5-2 in severe stress harris benedict to predict number of calories gut associated lymphoid tissue (GALT) propofol has 1.1 cal/cc
Alterations in GI motility is seen in the critically ill for a number of reasons: electrolytes, opioids, and alimentation.
Diarrhea approaches a 50% prevalence from medications, c. diff, alimentation, decreased luminal blood flow.
Malnutrition makes patients more difficult to wean, decreases respiratory and cardiac function, protein deficiency causes an acquired immunodeficiency,
Complications
Malnutrition is currently referred to as protein energy malnutrition (PEM)
Marasmus results from inadequate intake of calories
Kwashiorkor results from adequate calories but inadequate protein
The body undergoes a process of “autocannibalism” when under the acute stress of critical illness.
Fat was the preferred fuel for oxidation in the critically ill but it may be underutilized if provided in the U.S. form of linoleic acids.
Ideal would be alternate fat forms available in Europe like fish oil derived lipids.
Timing
well nourished patients can tolerate 7-10 days of semistarvation (weight loss of <10%) without adverse consequence.
However early enteral feeds (within 48 hours) is probably beneficial
Nutritional Requirements
Weight
Lean Body Weight=IBW + 0.4 (Actual weight – IBW)
IBW=50 kg + or 45 kg for females (2.3 kg for each inch over 60″)
use lean if pt obese or edematous
Caloric Requirements
Harris-Benedict
Basal Energy Expenditure (BEE)=66.5 + (13.7 x kg) + (5 x ht in cm) – (6.8 x age) in males
and 65.5 + (9.6 x kg) + (1.7 x ht) – (4.7 x age) in females
Resting EE=BEE x Stress Factor of 1.0-2.0
Total EE=REE x activity factor of 1.2-1.3 in a non-sedated, non-paralyzed patient
trauma 1.3, sepsis 1.6, burns 2.10
or if swan is in BEE=6.9 x VO2
25 total Kcal/kg ideal body weight can also be used to calculate minimum calorie requirement
65-70% as carbohydrate and 25-30% as fat
Do not count proteins in calories
1 Gram of
carbs=4 cals
Protein=3.4 cal
Fat=9 cal
Fat emulsion=10 cal
Protein
1.5 g/kg (IBW) of protein are needed per day
in severe trauma or burns, bump to 2.0
in CRF or hepatic disease reduce to 1.2 g/kg
can be provided as an essential amino acid formula in patients who can not take protein (liver/kidney)
Can keep increasing protein until bun bumps, though this may be a bit extreme
Electrolytes
Na 60-100 meq
K 60-100
Mg 10-20
Ca 10-15
Cl 80-120
Phos 20-30
If acidotic, acetate 0-60
also trace elements and vitamins
in burns, add zinc
Types of Formula
branched chain amino acids are helpful in liver failure patients
glutamine stimulates immune function
Ileostomy should put out <1 L per day. Consider tincture of opium.
Prealbumin
Prealbumin is produced by the choroid plexus, by pancreatic islet cells in the embryonic yolk sac, and by enterochromaffin cells in the gastrointestinal mucosa, but the liver is quantitatively the most important source.9 Liver production is maintained until late in liver disease. Hydration status does not affect prealbumin levels.5 A negative acute phase reactant, the prealbumin level will transiently decrease in the presence of inflammation and in the immediate postsurgical period. Serum levels also decline in patients with conditions associated with protein malnutrition, such as malignancy, cirrhosis, protein-losing enteropathy, and zinc deficiency
Clinical studies5 indicate that determination of the prealbumin level may allow for earlier recognition of and intervention for malnutrition. Prealbumin production decreases after 14 days of consuming a diet that provides only 60 percent of required proteins.10 Synthesis of prealbumin increases above baseline levels within 48 hours of protein supplementation in children with severe protein calorie malnutrition and returns to normal levels within eight days.6,11 These observations and others led to the recommendation that prealbumin levels should rise 2 g per dL (20 g per L) per day with adequate nutritional support.
Limitations of Using Prealbumin Level In acute alcohol intoxication, a leakage of proteins from damaged hepatic cells may cause a rise in the prealbumin level. Consequently, alcoholics may have elevated levels of prealbumin after binge drinking. A more realistic picture of the prealbumin level can be noted after one week, when levels return to baseline.15 Serum prealbumin levels may rise during prednisone therapy and in patients using progestational agents.16 Zinc deficiency may lower prealbumin levels, but vitamin deficiencies do not.10
Albumin reflects 21 days, transferrin 7-8 days, prealbumin 2 days
24 hour urine nitrogen balance study should ideally be 0-3
Nin=total in x conversion factor (6.25 for enteral, 6.06 for parenteral)
Nout=24 hour UUN in grams + 4 grams insensible loss
Balance=Nin-Nout
Metabolic cart measures energy expenditure Weir equation looks at heat combustion
VCO2/VO2 Lipolysis=0.7, overfed>1.1, Goal=0.8. If RQ<7 then it is usually a flawed study
pt should be resting for the 30 minutes prior to the study. Take calories that got you the 0.8 and give 1.3 X that amount as an activity factor.
BUN to protein ratio is 6.25
Prealbumin Risk Stratification
Prealbumin level Risk level<5.0 mg per dL (<50 mg per L) Poor prognosis 5.0 to 10.9 mg per dL (50 to 109 mg per L) Significant risk; aggressive nutritional support indicated 11.0 to 15.0 mg per dL (110 to 150 mg per L) Increased risk; monitor status biweekly 15.0 to 35.0 mg per dL (150 to 350 mg per L) Normal
If prealbumin levels are rising, it is likely that at least 65 percent of protein and energy needs are being provided
(Am Fam Phys April 15, 2002)
sr of early enteral nutrition for the critically ill (crit care med 2001;29(12):2264)
can feed patients even if they are on inotropes (Intensive Care Med 2001;27:540) though should probably be post-pyloric
Erythromycin dose of 70 mg accelerates gastric emptying as effectively as 200 mg in the critically ill (Intensive Care Medicine 2005;31:7)
This Article Abstract Full Text (PDF) Submit a response Alert me when this article is cited Alert me when eLetters are posted Alert me if a correction is posted Citation Map Services Email this article to a friend Similar articles in this journal Similar articles in PubMed Alert me to new issues of the journal Add to My Personal Article Archive Download to citation manager Google Scholar Articles by Artinian, V. Articles by DiGiovine, B. PubMed PubMed Citation Articles by Artinian, V. Articles by DiGiovine, B. (Chest. 2006;129:960-967.) © 2006 American College of Chest Physicians Effects of Early Enteral Feeding on the Outcome of Critically Ill Mechanically Ventilated Medical Patients* Vasken Artinian, MD, FCCP; Hicham Krayem, MD and Bruno DiGiovine, MD, MPH, FCCP * From the Department of Internal Medicine, Division of Pulmonary and Critical Care Medicine, Henry Ford Health System, Detroit, MI. Correspondence to: Bruno DiGiovine, MD, MPH, FCCP, Henry Ford Hospital, Division of Pulmonary and Critical Care, 2799 W Grand Blvd, K-17, Detroit, MI 48202; e-mail: bdigiov1@hfhs.org Abstract Study objectives: To determine the impact of early enteral feeding on the outcome of critically ill medical patients. Design: Retrospective analysis of a prospectively collected large multi-institutional ICU database. Patients: A total of 4,049 patients requiring mechanical ventilation for > 2 days. Measurements and results: Patients were classified according to whether or not they received enteral feeding within 48 h of mechanical ventilation onset. The 2,537 patients (63%) who did receive enteral feeding were labeled as the “early feeding group,” and the remaining 1,512 patients (37%) were labeled as the “late feeding group.” The overall ICU and hospital mortality were lower in the early feeding group (18.1% vs 21.4%, p = 0.01; and 28.7% vs 33.5%, p = 0.001, respectively). The lower mortality rates in the early feeding group were most evident in the sickest group as defined by quartiles of severity of illness scores. Three separate models were done using each of the different scores (acute physiology and chronic health evaluation II, simplified acute physiology score II, and mortality prediction model at time 0). In all models, early enteral feeding was associated with an approximately 20% decrease in ICU mortality and a 25% decrease in hospital mortality. We also analyzed the data after controlling for confounding by matching for propensity score. In this analysis, early feeding was again associated with decreased ICU and hospital mortality. In all adjusted analysis, early feeding was found to be independently associated with an increased risk of ventilator-associated pneumonia (VAP) developing. Conclusion: Early feeding significantly reduces ICU and hospital mortality based mainly on improvements in the sickest patients, despite being associated with an increased risk of VAP developing. Routine administration of such therapy in medical patients receiving mechanical ventilation is suggested, especially in patients at high risk of death.
Feeding Tubes
Multi-center RCT showed no benefit to NJ over NG (Crit Care Med 2012;40:2342)
If you need to know where corpack is, inject 50 cc of contrast and reshoot film
Residual volumes are a poor marker for aspiration risk (Crit Care Med 2005;33(2):324)
Jean Reignier et al. Effect of Not Monitoring Residual Gastric Volume on Risk of Ventilator-Associated Pneumonia in Adults Receiving Mechanical Ventilation and Early Enteral Feeding. A Randomized Trial. JAMA. 2013;309(3):249-256.
Feed early and enterally if possible Aim for an energy intake of 25 kcal/kg/d Aim for a protein intake of 1.2 g/kg/d
In a person who is eating normally and in a person who is starving, provision of energy (glucose) suppresses gluconeogenesis completely. This is true also in a person with mild injury or mild sepsis.8 But in a patient with severe sepsis or injury, provision of energy (glucose) suppresses gluconeogenesis only partially, even at maximum rates of glucose provision of 5 mg/kg/min. Therefore, the provision of energy to severely septic or injured patients will never preserve lean tissue mass.9 The most that you can hope to achieve is to slow down the rate at which lean tissue is lost. Protein, given in the form of intravenous amino acids, affects protein metabolism. A healthy person has a protein intake of 1 g/kg/24h. Protein given to a severely septic patient at rates of 1.2 g/kg/24h diminishes net breakdown of protein.
Both protein synthesis and breakdown are stimulated by giving protein, but synthesis more so than breakdown, resulting in a net reduction in breakdown of protein. However, if you give protein at a rate of 2 g/kg/24h, breakdown is stimulated more than synthesis and protein oxidation is increased even more. Provision of nutritional support at rates higher than 4-5 mg/kg/min for glucose and 1.5-2.0 g/kg/24h for protein will have no effect on the rates of lean tissue loss in the severely septic or injured patient. To do so, results in overstimulation of metabolism (energy expenditure, carbon dioxide production, protein oxidation) and stresses the patient’s system even further. Improvements in surrogate end points (wound healing and muscle function) have been demonstrated with short term (24-48 hours) nutritional support.10 11 But these have not been translated into clinically relevant benefits until feeding has been maintained for more than five days.12
Because gastric secretions between 80 ml/h and 125 ml/h are normal, withholding feed for gastric residual volumes less than 400 ml may not have physiological relevance.49 Importantly, no studies to date have demonstrated that using lower values of gastric residual volumes correlates with a decreased risk of aspiration.48
Method to pass tubes (Inten Care Med 2006;32:553)
The Corpak 10-10-10 protocol for blind insertion of nasojejunal
feeding tubes at the bedside.
1. Unless clinically contraindicated, 10 mg metoclopramide
is given by slow intravenous injection (if
not given in the preceding 4 h). Allow 10 min after
the metoclopramide before commencing tube
placement.
2. Lubricate the end of the fine bore feeding tube with
aqueous gel.
3. Measure the tube from the patients nose, via the ear,
down to the xiphoid process.
4. Ideally place the patient in a semi-supine position at
30°.
5. Advance the tube via the nostril, aiming the tip parallel
to the nasal septum and superior surface of hard
palate, into the nasopharynx, until the previously measured
length (approx. 40 cm) is reached.
6. Confirm placement in the stomach.
7. Flush the tube with 1 ml 0.9% saline to lubricate the
wire within the tube.
8. Advance the tube further by continued gentle pushing,
pulling back if any resistance is felt, until a further
15 cm of tube has been advanced. Check tube passage.
9. To do this the guide wire should be pulled back a little
way (no more than 5 cm). If resistance is met when
pulling back the guide wire then the tube is likely to be
coiled in the stomach. This resistance can be characterized
with the feeling that the guide wire is popping
when it is pulled back.
10. If the tube is coiled, pull it back slowly 5 cm at a time
until the wire can be manipulated freely.
11. Continue to advance the tube again slowly but again
check at 70, 75, 80, 85, 90 and 95 cm to ensure that the
tube has not become coiled. Follow steps 9 and 10.
12. Once the 95-cm point has been reached without the
tube becoming coiled, the tube can be advanced slowly
to 105 cm to ensure successful placement in the jejunum.
13. If the procedure has been underway for more than
20 min, 200 ml air should be insufflated into the
stomach via the NG tube. Further attempts to pass the
tube should be made for 20 min.
14. Final tube placement confirmation:
If on aspiration there is a high volume of air
(
> 20 ml) it is likely that the tube remains in
either the oesophagus or the upper portion of the
stomach.
If on aspiration 20ml or more of secretions is obtained,
the tube is most likely to be in the stomach.
These secretions usually have a pH
< 5.0.
If no more than 510 ml bright yellow secretions is
obtained, the tube is likely to be in the small bowel.
Secretions from the small bowel should be pH 67.
If no secretions are obtained, bolus 10 ml air down
the tube. If on attempted aspiration resistance is
met, the tube can be judged to be in the small
bowel.
Flush the tube with 10 ml 0.9% saline. If less than
5 ml can be aspirated easily, the tube is likely to be
in the small bowel.
15. Remove the guide wire. If the wire has maintained its
smooth appearance, the tube can be judged to be in the
small bowel. Secure the tube to the side of the patients
head.
16. Request confirmation of placement by upper abdominal
radiography. The tube is radio-opaque even with
the guidewire removed. The tube is seen to cross the
midline from patients left to right, and then to cross
again from right to left if placement into the jejunum
has been successful.
17. Once placement has been confirmed, restart feeding via
the NG route. Leave the NG tube in situ and aspirate it
4 hly to identify reflux of feed, back into the stomach.
(
(Critical Care Medicine:Volume 37(2)February 2009pp 523-527) Preparation and Positioning. TOP
Patients were administered 10-mg metoclopramide intravenously before tube insertion. The patient was placed supine with the head of the bed raised at 30-45°. The tube was looped behind the patient’s ear, and the distance from the tip of the ipsilateral nostril to the xiphisternum was measured as an estimate of the depth of insertion necessary for the tube tip to lie within the stomach. The feeding tube was then lubricated with aqueous gel.
Esophageal Placement. TOP
Cooperative patients with an intact gag reflex were asked to take a sip of water and keep this in the mouth. The tube was then passed into the nostril, parallel to the hard palate. As soon as the tube touched the back of the nasopharynx, the patient was asked to swallow while the tube was simultaneously advanced to 35-40 cm. At this level, esophageal placement was confirmed by a combination of air insufflation with auscultation in the epigastrium (the whoosh test) (7) and by assessing for coiling using the indwelling guide wire. If doubt still existed as to esophageal placement, laryngoscopy was performed in unconscious patients to exclude the possibility of tracheobronchial intubation. Finally, if placement in the esophagus could not be confirmed, the tube was withdrawn back into the nose, and further attempts at esophageal placement were made.
Gastric Placement. TOP
The tube was advanced into the stomach, as guided by measurements taken before tube insertion. This level invariably lay at between 55 and 65 cm. Starting at 40 cm, aspiration was attempted at 5-cm intervals till the required intragastric position was established. Aspiration with a 20-mL syringe was attempted three times at each level. Air insufflation and patient turning were used if aspiration failed. Confirmation of gastric placement was again performed using the whoosh test and then by instilling and reaspirating 100 mL of air. This latter vacuum test maneuver (8) is possible only in the large volume of the stomach. Any fluid aspirate was tested for pH, and assessment for coiling was also performed using the guide wire.
Postpyloric Placement. TOP
Postpyloric placement was achieved by advancing the tube at 5-cm intervals and checking its position at each stage without other delays between 5-cm intervals. In this manner, the tube was advanced to 115 cm such that the tube tip lay at or beyond the duodenojejunal flexure. Placement was checked at each 5 cm by the insufflation of 100 mL of air, which resulted in a minimal return of air on aspiration (usually <20 mL using a 20-mL syringe), once the tube had passed the pylorus (the vacuum test). Any fluid aspirate obtained was checked for pH (8), and the guide wire was also used to assess tube tip placement.
The main difficulty encountered at this stage was coiling of the tube in the stomach (Fig. 2a). In a coiled tube, an indwelling guide wire can be withdrawn with ease but cannot be readvanced without some force (9). This subjective catching sensation is a fundamental part of the learning curve for this technique as it suggests coiling and was used to indicate the need to withdraw the tube back to 55 cm for further attempts at pyloric intubation.
Figure 2. Plain abdominal radiographs showing a nasojejunal tube that has coiled in the stomach (a) and one where the tip is positioned beyond the duodeno-jejunal flexure (b). The latter also demonstrates the classic C-shaped duodenal configuration diagnostic of postpyloric placement.
Once the required position was achieved, the tube was secured to the nose with adhesive tape, and correct placement was confirmed radiologically before starting the feed (Fig. 2b). Radiographs were interpreted independently by two consultant radiologists, and the placement of the tube tip at different levels was recorded as lying at the level of D1-D4 (first to fourth part of the duodenum) or at or beyond the duodenojejunal flexure.
Early enteral immunonutrition as compared to parenteral was much better for incidence of sepsis and ICU Length of stay (Inten Care Med 2006;32:1191)
feeding with acids and antioxidants results in better outcomes in sepsis (Crit Care Med 2006;34:2325)
Trophic and full feeds seem to have same outcomes early on in patients with acute resp failure (Crit Care Med 2011;39:967)
Open Bellies
It may be reasonable to start trophic feeds if the pt doesn’t have bowel injuries from the WEST (Journal of Trauma and Acute Care Surgery Issue: Volume 73(6), December 2012, p 1378–138)
Gastric Residuals
Newest RCT of Early PN
Early Parenteral Nutrition in Critically Ill Patients With Short-term Relative Contraindications to Early Enteral NutritionA Randomized Controlled Trial FREE Gordon S. Doig, PhD; Fiona Simpson, MND; Elizabeth A. Sweetman, MHM; Simon R. Finfer, FCICM; D. Jamie Cooper, FCICM; Philippa T. Heighes, MN; Andrew R. Davies, FCICM; Michael O’Leary, FCICM; Tom Solano, FCICM; Sandra Peake, FCICM; for the Early PN Investigators of the ANZICS Clinical Trials Group [+] Author Affiliations JAMA. 2013;309(20):2130-2138. doi:10.1001/jama.2013.5124. Text Size: A A A