
irrigation foley technique (J Trauma 2008;64:1159)
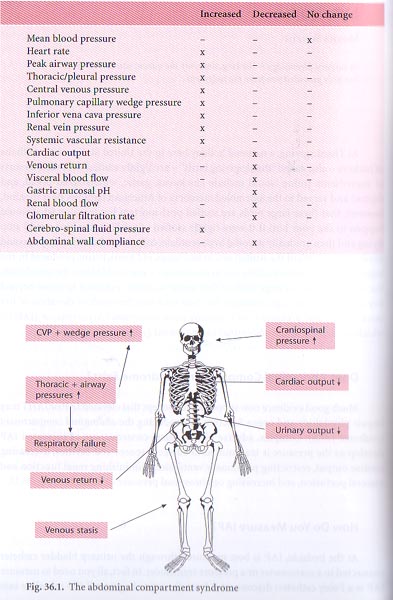
abdominal hypertension is a condition of increased intrabdominal pressure, in its later stages, it causes abdominal compartment syndrome compressing vasculature and organs.
mild=10-20 mm Hg
moderate=21-30 mm Hg
severe=>30 requiring operative intervention in all cases
burr closure or star closure device allows the sewing of two sheets of velcro to wound edges allowing the wound edges to be drawn together and preventing sideward retraction.
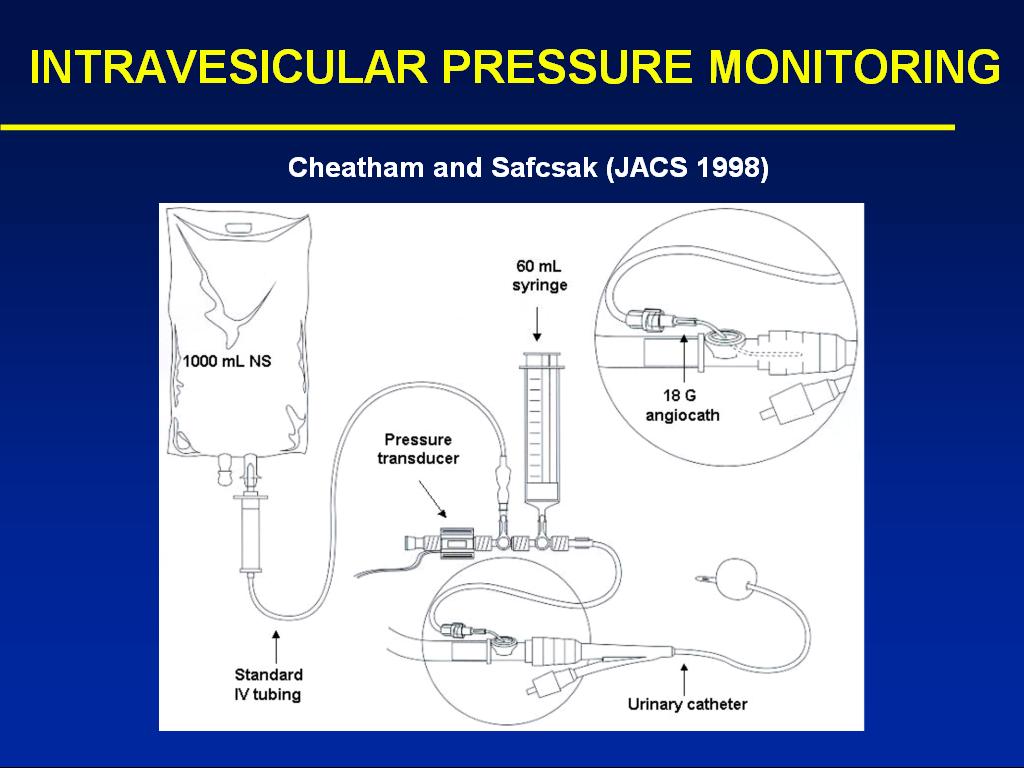
Hold foley tubing straight up from symphysis pubis, height of urine column is the pressure. If there is no urine, instill 100 cc of saline. Comparable accuracy to other standard techniques. (J Trauma 2002, 52:1169)
Can be caused by ascites
How to measure bladder pressure:
IAH review (Curr Opin Crit Care 2005;11:1156)
measure bladder pressure at end exp in supine position. zero at mid ax line
Hg to Cm H2O is 1.36, H2O to Hg is 0.74
APP=MAP-IAP
Most recent Consensus Definitions from World Society of ACS (www.wsacs.org)
Consensus Definitions & Recommendations
The WSACS solicits your comments and recommendations regarding the following proposed consensus definitions on intra-andominal hypertension (IAH) and abdominal compartment syndrome (ACS).
DEFINITIONS
Intraabdominal Pressure (IAP):
- Intraabdominal pressure (IAP) is the pressure concealed within the abdominal cavity. IAP varies with respiration.
- Normal IAP is approximately 5 mmHg, but can be non-pathologically increased in the obese.
- IAP should be expressed in mmHg (1 mmHg = 1.36 cmH2O) and measured at end-expiration in the supine position.
- Abdominal muscle contractions should be absent
- The transducer should be zeroed at the level of the mid-axillary line
- The gold standard for direct IAP measurement is via direct needle puncture and transduction of the pressure within the abdominal cavity (eg. during peritoneal dialysis or laparoscopy).
- The gold standard for intermittent indirect IAP measurement is via transduction of the pressure within the bladder.
- The gold standard for continuous indirect IAP measurement is via a balloon-tipped catheter in the stomach or via a continuous bladder irrigation method.
- Abdominal perfusion pressure (APP) = mean arterial pressure (MAP) – IAP.
- Filtration gradient (FG) = glomerular filtration pressure (GFP) – proximal tubular pressure (PTP) = MAP – 2 * IAP.
Intra-abdominal Hypertension (IAH):
- IAH is defined by either one or both of the following:
- An IAP > 12 mmHg, recorded by a minimum of two standardized measurements conducted 4-6 hours apart.
- An APP < 60 mmHg, recorded by a minimum of two standardized measurements conducted 1-6 hours apart.
- IAH is graded as follows: Grade Intraabdominal Pressure (IAP) I 12-15 mmHg II 16-20 mmHg III 21-25 mmHg IV > 25 mmHg
- According to the duration of symptoms, IAH can be further classified into 4 groups:
- Chronic IAH
- Acute IAH
- Subacute IAH
- Hyperacute IAH
Abdominal Compartment Syndrome (ACS):
- ACS is defined as the presence of BOTH:
- An IAP > 20 mmHg with or without APP < 50 mmHg recorded by a minimum of three standardized measurements conducted 1-6 hours apart AND;
- Single or multiple organ system failure which was not previously present
- In contrast to IAH, ACS should not be graded as it is an all or nothing phenomenon.
- Primary ACS refers to:
- A condition associated with injury or disease in the abdomino-pelvic region that frequently requires early surgical or angioradiological intervention, OR
- A condition that develops following abdominal surgery (such as abdominal organ injuries that require surgical repair or damage control surgery, secondary peritonitis, bleeding pelvic fractures or other cause of massive retroperitoneal hematoma, liver transplantation).
Patients that undergo an initial trial of nonoperative management for solid organ injuries who subsequently develop ACS are included in the Primary ACS category.
Former synonyms include “abdominal”, “surgical” or “acute”.
- Secondary ACS refers to:
- Conditions that do not originate from the abdomen (such as sepsis and capillary leak, major burns, and other conditions requiring massive fluid resuscitation), yet result in the signs and symptoms commonly associated with Primary ACS.
Former synonyms = “extra-abdominal”, “medical” or “subacute”.
- Tertiary or Recurrent ACS refers to:
- A condition in which ACS develops following prophylactic or therapeutic surgical or medical treatment of Primary or Secondary ACS (e.g. persistence of ACS after decompressive laparotomy or development of a new ACS episode following definitive closure of the abdominal wall after the previous utilization of a temporary abdominal wall closure)
Former synonyms = “chronic” or “open”.
- To differentiate between localised and systemic IAH/ACS the bladder-to-gastric pressure difference should be measured. A localised problem is present when this difference exceeds 10 mmHg.
RECOMMENDATIONS
- Scientific studies examining the prevalence and incidence of IAH/ACS should be based on the above sited definitions and classifications.
- Results should be provided for mean, median, and maximal IAP values on admission and during the study stay.
- Evaluation of IAP thresholds should be based upon the analysis of receiver operating characteristics (ROC) and the area under the ROC curve.
- Studies examining new devices to measure IAP should always compare the new IAP measurement method to one of the accepted gold standard methods.
- Validation of a new technique should not be limited to the analysis of significant correlation coefficients with R2, but should also include an analysis according to Bland and Altman .
- The presence of IAH/ACS whether primary, secondary or tertiary should always be viewed in the context of the underlying etiologies. We identify 4 major patient categories:
- Surgical
- Medical
- Trauma
- Burn
ADDENDUM
Examples of appropriate classification:
Classification Patient DescriptionChronic, primary, medical, grade II IAH A patient with chronic liver failure complicated with variceal bleeding and cardiorespiratory collapse and an IAP of 18 mmHg Subacute, secondary, trauma, grade III IAH A patient with penetrating cardiac injury, presenting with cardiorespiratory collapse requiring massive resuscitation develops an increased IAP above 21 mmHg on the third day of hospitalisation Acute, secondary, medical, grade I IAH A patient with a septic shock related to a pneumonia has an IAP of 13 mmHg on admission Acute, primary, medical, grade IV IAH A patient with a septic shock due to localised intestinal perforation and an IAP of 25 mmHg Subacute, primary, burn, grade III IAH A burn patient with a big abdominal eschar develops an IAP above 20 mmHg on day 7 Acute, primary, medical, localised grade IV IAH A patient with chronic renal failure and on low molecular weight heparins develops a rectus sheath and psoas hematoma with localised pressure on the bladder and kidneys, the bladder-to-gastric pressure difference is 25 minus 10 mmHg or thus 15 mmHg
Underlying predisposing conditions for IAH:
- Acidosis defined as an arterial pH below 7.2
- Hypothermia defined as a core temperature below 33°C
- Polytransfusion defined as the transfusion of more than 10 Units of Packed Red Cells in a 24 hour period
- Coagulopathy defined as a platelet count below 55000/mm3 or an activated partial thromboplastin time (APTT) more than 2 times normal or a prothrombin time (PTT) below 50% or an international standardised ratio (INR) more than 1.5
- Sepsis defined according to the American – European Consensus Conference definitions
- Bacteraemia defined as the presence of bacteria in the bloodstream determined by blood cultures
- Liver dysfunction defined as decompensated or compensated cirrhosis or other liver failure with ascites (paraneoplastic, cardiac failure, portal vein thrombosis, ischemic hepatitis)
- Mechanical ventilation
- Use of positive end expiratory pressure (PEEP) or the presence of auto-PEEP
- Pneumonia as defined according to standard criteria
Etiologic factors for IAH:
- Abdominal surgery
- laparoscopy
- reduction of hernia, tight closure
- abdominal banding with postoperative Velcro belt to prevent incisional hernia
- Massive fluid resuscitation defined as more than 5 litres of colloids or crystalloids in a 24 hour period
- Ileus whether paralytic, mechanical or pseudo-obstructive defined as abdominal distension or absence of bowel sounds or failure of enteral feeding; evidenced by gastric dilatation or massive gastroparesis with a gastric residual of more than 1000mL in a 24 hour period
- Abdominal infection (pancreatitis, peritonitis, abscess, )
- Pneumoperitoneum
- Haemoperitoneum either caused by an intra- or retroperitoneal bleeding
Indications for IAP monitoring:
- Postoperative patients (abdominal surgery)
- Patients with open or blunt abdominal trauma
- Mechanically ventilated ICU Patients with other organ dysfunction as assessed by daily Sequential Organ Failure Assessment (SOFA) score
- Patients with a distended abdomen and signs and symptoms consistent with abdominal compartment syndrome
- Oliguria
- Hypoxia
- Hypotension
- Unexplained acidosis
- Mesenteric ischemia
- Elevated ICP
- Patients with abdominal packing after temporary abdominal closure for multiple trauma or liver transplantation
- Patients with open abdomens, especially if they have an IV bag closure and are in the early post-operative period, may still develop abdominal compartment syndrome
- Patients who have not had an operation but have received large volumes of fluid resuscitation in the context of an underlying capillary leak problem (pancreatitis, septic shock, trauma, etc.)
Nonsurgical treatment options:
- Paracenthesis
- Gastric suctioning
- Rectal enemas and suctioning
- Gastroprokinetics (cisapride, metoclopramide, domperidone, erythromycin)
- Colonoprokinetics (prostygmine)
- Furosemide either alone or in combination with human albumin 20%
- Continuous venovenous hemofiltration with aggressive ultrafiltration
- Continuous negative abdominal pressure
- Sedation
- Curarisation
- Body positioning
Intra-abdominal hypertension Intra-abdominal hypertension (IAH) is defined by either one or both of the following: (1) an IAP of 12 mm Hg or greater, recorded by a minimum of three standardized measurements conducted 4 to 6 hours apart; (2) an APP of 60 mm Hg or less, recorded by a minimum of two standardized measurements conducted 1 to 6 hours apart. IAH is graded as shown in Table 1. Abdominal compartment syndrome Abdominal compartment syndrome is defined as the presence of an IAP of 20 mm Hg or greater with or without APP below 50 mm Hg, recorded by a minimum of three standardized measurements conducted 1 to 6 hours apart and single or multiple organ system failure that was not previously present. In contrast to IAH, ACS should not be graded because it is an all-or-nothing phenomenon.
The precise management of IAP remains somewhat clouded by many published anecdotal reports and uncontrolled series. Aggressive nonoperative intensive care support is critical to prevent the complications of ACS. This involves careful monitoring of the cardiorespiratory system and aggressive intravascular fluid replacement, especially if this is associated with hemorrhage [30]. Excessive fluid resuscitation, however, will actually add to the problem [31]. Simple measures such as nasogastric decompression are, of course, mandatory. Some possible nonsurgical options are these: (1) Paracentesis; (2) Gastric suctioning; (3) Rectal enemas and suctioning; (4) Gastroprokinetics (cisapride, metoclopramide, domperidone, erythromycin); (5) Colonoprokinetics (prostigmine); (6) Furosemide either alone or in combination with human albumin 20%; (7) Continuous venovenous hemofiltration with aggressive ultrafiltration; (8) Continuous negative abdominal pressure; (9) Sedation; (10) Curarization; (11) Body positioning; (12) Botulinum toxin into internal anal sphincter.
Measure at phlebostatic axis in supine patient, not at the pubic symphysis
Case Report of Paracentesis for ACS in burn pts (J Trauma 2006;60:1119)
Consensus Definitions (Inten Care Med 2006;32:1722)
Definition 1 IAP is the steady-state pressure concealed within the abdominal cavity. Definition 2 APP = MAP − IAP. Definition 3 FG = GFP − PTP = MAP − 2 × IAP. Definition 4 IAP should be expressed in mmHg and measured at end-expiration in the complete supine position after ensuring that abdominal muscle contractions are absent and with the transducer zeroed at the level of the midaxillary line. Definition 5 The reference standard for intermittent IAP measurement is via the bladder with a maximal instillation volume of 25 ml sterile saline. Definition 6 Normal IAP is approx. 57 mmHg in critically ill adults. Definition 7 IAH is defined by a sustained or repeated pathological elevation in IAP ≥ 12 mmHg. Definition 8 IAH is graded as follows: grade I, IAP 1215 mmHg; grade II, IAP 1620 mmHg; grade III, IAP 2125 mmHg, grade IV, IAP > 25 mmHg. Definition 9 ACS is defined as a sustained IAP > 20 mmHg (with or without an APP < 60 mmHg) that is associated with new organ dysfunction/failure. Definition 10 Primary ACS is a condition associated with injury or disease in the abdominopelvic region that frequently requires early surgical or interventional radiological intervention. Definition 11 Secondary ACS refers to conditions that do not originate from the abdominopelvic region. Definition 12 Recurrent ACS refers to the condition in which ACS redevelops following previous surgical or medical treatment of primary or secondary ACS.
Perc drainage works for relieveing ACS (CHEST December 2011vol. 140 no. 6 1428-1435)